
Key Takeaways
- Trematode-associated uveitis (TAU) is a granulomatous, usually unilateral intraocular inflammation linked to freshwater exposure in endemic tropical and subtropical regions.
- Pearl-like white nodules in the anterior chamber or on the iris — especially in children — are the single most characteristic clue.
- It is frequently misdiagnosed as idiopathic anterior uveitis or endophthalmitis, so a careful exposure history is central to the diagnosis.
- Inflammation is largely immune-mediated: corticosteroids alone often fail, and surgical excision of granulomas helps selected cases.
- Routine systemic antiparasitic therapy is not universally recommended and should be individualized.
Last updated: July 2026 · Reviewed for clinical accuracy by the Choroida Ophthalmology Education team. This article is written for eye-care professionals and is not a substitute for individualized clinical judgment.

Uveitis is a diverse group of inflammatory eye diseases with infectious, autoimmune, traumatic, and idiopathic causes. While viral, bacterial, fungal, and protozoal infections are well recognized in ophthalmic practice, parasitic infections remain an overlooked cause of ocular inflammation in many parts of the world.
Among these, trematode-associated uveitis (TAU) is an emerging and often underrecognized clinical entity, reported predominantly in tropical and subtropical regions where freshwater exposure is common. Because its presentation may mimic idiopathic anterior uveitis, endophthalmitis, or other inflammatory disorders, delayed diagnosis is frequent.
Early recognition matters because conventional anti-inflammatory therapy alone is often insufficient, and prolonged inflammation can lead to irreversible ocular complications. For ophthalmologists practicing in endemic areas, a high index of suspicion for trematode-associated uveitis can be vision-saving.
What Is Trematode-Associated Uveitis?
Trematode-associated uveitis is an intraocular inflammatory disorder believed to result from infection by trematode (fluke) parasites, or from an immune-mediated response to parasitic antigens. Most reported cases are associated with exposure to freshwater inhabited by snails that serve as intermediate hosts in the parasite’s life cycle.
The disease most commonly affects:
- Children
- Young adults
- Individuals with frequent freshwater exposure
- Residents of endemic rural communities
👉 In endemic regions, a history of swimming or bathing in canals, rivers, or lakes is an important diagnostic clue.
Epidemiology
Although considered uncommon globally, trematode-associated uveitis has been increasingly recognized in:
- Egypt
- Sudan
- Saudi Arabia
- India
- Southeast Asia
- Other tropical regions
Clusters of cases have been described, particularly among children following recreational freshwater exposure. Because many cases are initially misdiagnosed as idiopathic uveitis, the true prevalence is likely underestimated.
Pathogenesis
The exact mechanism remains incompletely understood, and two major hypotheses have been proposed.
1. Direct Parasitic Involvement
The parasite or its larval forms may enter ocular tissues, triggering local inflammation.
2. Immune-Mediated Response
More commonly, inflammation appears to result from a hypersensitivity reaction against trematode antigens rather than active intraocular infection. Inflammation may involve the iris, ciliary body, vitreous, retina, and choroid.
👉 Many experts believe that immune-mediated inflammation plays a greater role than direct parasitic invasion in most cases.
Risk Factors
Several historical features should increase clinical suspicion.
Environmental Risk Factors
- Swimming in freshwater canals
- River bathing
- Agricultural water exposure
- Living in endemic rural areas
- Contact with snail-infested water
Patient Factors
- Young age
- Male predominance in some studies
- Recurrent unilateral uveitis
- Lack of systemic autoimmune disease
A careful environmental history is often the key to diagnosis.
Clinical Presentation
Most patients present with acute or subacute unilateral inflammation.
Common Symptoms
- Blurred vision
- Ocular redness
- Eye pain
- Photophobia
- Floaters
Visual acuity may range from mildly reduced to severely impaired, depending on the degree of inflammation and posterior segment involvement.
Slit-Lamp Examination Findings
The anterior segment frequently demonstrates:
- Granulomatous anterior uveitis
- Large “mutton-fat” keratic precipitates
- Anterior chamber cells and flare
- Posterior synechiae
- Iris nodules in selected cases
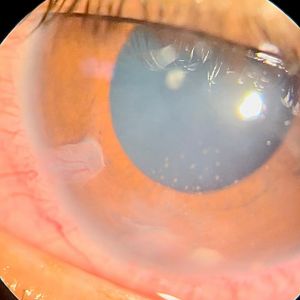
One of the most characteristic findings is the presence of pearl-like white nodules within the anterior chamber or attached to the iris, particularly in pediatric cases.
👉 Anterior chamber pearl-like granulomas are considered highly suggestive of trematode-associated uveitis in endemic regions.
Posterior Segment Findings
Although anterior uveitis predominates, posterior involvement may occur. Possible findings include:
- Vitritis
- Retinal vasculitis
- Choroiditis
- Macular edema
- Optic disc edema
Posterior disease generally indicates more severe inflammation.
Differential Diagnosis
Several conditions can closely resemble trematode-associated uveitis. The table below summarizes the most useful distinguishing clues.
| Condition | Key clue that argues against TAU |
|---|---|
| Sarcoidosis | Often bilateral; systemic involvement, elevated ACE, hilar lymphadenopathy |
| Tuberculous uveitis | Positive TB testing; broad or serpiginous-like choroiditis; endemic TB exposure |
| Ocular toxocariasis | Peripheral or posterior granuloma / mass; positive Toxocara serology |
| Toxoplasmosis | Focal necrotizing retinochoroiditis beside an old scar (“headlight in the fog”) |
| JIA-associated uveitis | Chronic bilateral non-granulomatous uveitis with arthritis; ANA-positive |
| Endogenous endophthalmitis | Systemically ill patient; rapid progression; positive cultures |
| Intraocular lymphoma | Older patient; steroid-resistant vitritis; CNS involvement |
👉 Geographic location and exposure history are often critical for narrowing the diagnosis.

Diagnostic Evaluation
No single laboratory test confirms every case. Diagnosis relies on a combination of clinical findings, exposure history, imaging, and exclusion of other causes.
Laboratory Investigations
May include:
- Complete blood count
- Eosinophil count
- Stool examination for parasites
- Serologic testing when appropriate
- Tuberculosis screening
- Syphilis testing
Most laboratory investigations primarily help exclude alternative diagnoses.
The Role of Imaging
Optical Coherence Tomography (OCT)
Useful for detecting:
- Cystoid macular edema
- Epiretinal membranes
- Vitreomacular interface abnormalities
Fluorescein Angiography
May demonstrate retinal vascular leakage, disc leakage, macular edema, and areas of retinal vasculitis. For a broader review of how to read leakage patterns, see our article on leaky vessels on angiography.
B-Scan Ultrasonography
Helpful when media opacity limits posterior segment visualization.
Management
Treatment depends on the severity and stage of inflammation.
Corticosteroids
Topical corticosteroids remain the mainstay for anterior segment inflammation. Severe cases may require periocular or systemic corticosteroids. However, steroids alone may not provide lasting control.
Cycloplegic Agents
Cycloplegics help relieve pain, prevent posterior synechiae, and stabilize the blood-aqueous barrier.
Surgical Management
In selected patients, surgery may be indicated. Procedures include removal of anterior chamber granulomas, pars plana vitrectomy, and cataract extraction when necessary. Surgical excision of pearl-like granulomas has been associated with favorable outcomes in carefully selected cases.
👉 Persistent anterior chamber nodules despite medical therapy may require surgical removal.
Antiparasitic Therapy
The role of systemic antiparasitic medications remains controversial. Current evidence suggests that active intraocular parasites are rarely identified, and that many patients improve primarily with anti-inflammatory therapy and surgical management when indicated. Routine antiparasitic treatment is therefore not universally recommended and should be individualized based on the clinical scenario and infectious disease consultation.
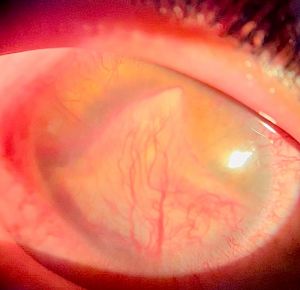
Potential Complications
Untreated or recurrent inflammation may result in:
- Cataract
- Secondary glaucoma
- Band keratopathy
- Posterior synechiae
- Chronic cystoid macular edema
- Epiretinal membrane
- Permanent vision loss
Early intervention substantially reduces the risk of these complications.
Prognosis
Visual prognosis depends on early diagnosis, the severity of inflammation, the presence of posterior segment involvement, and the development of complications.
Most patients experience favorable outcomes with timely diagnosis and appropriate management. Delayed diagnosis, however, increases the likelihood of chronic inflammation and irreversible structural damage.
Future Perspectives
Greater awareness of trematode-associated uveitis is leading to improved recognition in endemic regions. Current areas of research include:
- Molecular diagnostic techniques
- Improved parasite identification
- Immunopathogenesis
- Biomarkers of disease activity
- Standardized treatment protocols
These advances may facilitate earlier diagnosis and more targeted therapy.
Frequently Asked Questions
What causes trematode-associated uveitis?
It is caused by trematode (fluke) parasites, or by an immune-mediated response to their antigens, typically after exposure to freshwater in endemic tropical regions.
What is the hallmark clinical sign?
Pearl-like white nodules in the anterior chamber or on the iris — most often seen in children — are the most characteristic finding.
How is trematode-associated uveitis diagnosed?
There is no single confirmatory test. Diagnosis combines clinical findings, a freshwater exposure history, imaging (OCT, fluorescein angiography, B-scan), and exclusion of other causes of granulomatous uveitis.
Is antiparasitic treatment always required?
No. Active intraocular parasites are rarely identified, so routine antiparasitic therapy is not universally recommended. Management centers on anti-inflammatory treatment and, in selected cases, surgical removal of granulomas.
Which regions report the most cases?
Egypt, Sudan, Saudi Arabia, India, Southeast Asia, and other tropical and subtropical regions, usually after recreational freshwater exposure.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is a new advancement in the field of science and technology, in which photographs of the desired slit-lamp finding can be captured with a smartphone by using a slit-lamp adapter.
Slit-lamp Smartphone photography
References
- Abdelazeem K, et al. “Presumed trematode-induced granulomatous anterior uveitis in Egyptian children: clinical features and outcomes.” Ocular Immunology and Inflammation. 2015.
- El-Gayar EK, et al. “Trematode-induced uveitis: clinical spectrum and management.” Journal of Ophthalmic Inflammation and Infection. 2019.
- Herbort CP Jr, Rao NA, Mochizuki M. “International criteria for the diagnosis of ocular inflammatory diseases.” Ocular Immunology and Inflammation. 2021.
- Nussenblatt RB, Whitcup SM. Uveitis: Fundamentals and Clinical Practice. 5th Edition. Elsevier.
- Jabs DA, et al. “Standardization of Uveitis Nomenclature (SUN) Working Group classification criteria.” Am J Ophthalmol. 2021.
- Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach. 9th Edition.

{kind=link}