
Pediatric glaucoma surgery presents unique challenges that differ substantially from glaucoma procedures performed in adults.

Congenital and childhood glaucomas often require early surgical intervention to preserve vision and prevent irreversible optic nerve damage.
Procedures such as trabeculotomy, goniotomy, trabeculectomy, glaucoma drainage device implantation, and combined surgeries have significantly improved long-term outcomes in these patients.
Although most pediatric glaucoma surgeries are successful, surgeons must remain vigilant for rare but potentially devastating complications.
Among these, suprachoroidal hemorrhage (SCH) is one of the most feared. Characterized by the accumulation of blood within the potential space between the choroid and sclera, SCH can lead to sudden intraoperative or postoperative vision loss and may threaten both anatomical and functional outcomes.
Fortunately, suprachoroidal hemorrhage is considerably less common in children than in adults. However, when it occurs, prompt recognition and appropriate management are essential to maximize the chance of visual recovery.
For pediatric glaucoma surgeons, understanding the risk factors, early warning signs, and management principles of SCH is critical despite its rarity.
What Is Suprachoroidal Hemorrhage?
Suprachoroidal hemorrhage occurs when blood accumulates within the suprachoroidal space due to rupture of the long or short posterior ciliary vessels.
The hemorrhage may be:
- Limited and localized
- Massive and circumferential
- Intraoperative
- Delayed postoperative
Depending on its severity, SCH may produce:
- Sudden shallowing of the anterior chamber
- Marked elevation of intraocular pressure (IOP)
- Retinal apposition (“kissing choroidals”)
- Retinal detachment
- Permanent vision loss
Rapid recognition during surgery can significantly influence the final outcome.
Why Is SCH Less Common in Children?
Compared with adults, children generally have:
- More elastic scleral tissue
- Healthier choroidal vasculature
- Lower prevalence of systemic vascular disease
- Less age-related vascular fragility
These characteristics likely contribute to the lower incidence of SCH in pediatric glaucoma surgery.
However, pediatric eyes possess unique anatomical features—including lower scleral rigidity and more dynamic ocular pressure changes—that can make intraoperative hypotony particularly challenging.
Pathophysiology
The development of SCH is usually triggered by sudden hypotony.
Rapid reduction in intraocular pressure causes:
- Choroidal expansion
- Stretching of posterior ciliary vessels
- Vascular rupture
- Accumulation of blood in the suprachoroidal space
As the hemorrhage enlarges, it may further increase intraocular pressure, creating a vicious cycle of ocular compression and ischemia.
Acute hypotony remains the single most important initiating event in most cases of SCH.
Risk Factors in Pediatric Glaucoma Surgery
Although evidence is limited because of the rarity of the condition, several factors are believed to increase risk.
Surgical Risk Factors
- Sudden decompression of markedly elevated IOP
- Excessive intraoperative hypotony
- Difficult anterior chamber maintenance
- Combined glaucoma procedures
- Prolonged surgical time
- Repeat glaucoma surgery
Maintaining stable intraocular pressure throughout surgery is one of the most important preventive strategies.
Ocular Risk Factors
Certain ocular characteristics may predispose to SCH.
These include:
- Buphthalmos
- High axial myopia
- Previous intraocular surgery
- Aphakia
- Aniridia
- Severe congenital glaucoma with stretched ocular coats
Eyes with abnormal anatomy may be more susceptible to rapid pressure fluctuations.
Systemic Risk Factors
Systemic factors play a smaller role in children than in adults but may include:
- Coagulation disorders
- Blood dyscrasias
- Anticoagulant therapy (rare in pediatric patients)
- Severe hypertension in older children
Whenever possible, systemic abnormalities should be identified before surgery.
When Can SCH Occur?
Intraoperative SCH
This is the most dramatic presentation.
It often occurs immediately after:
- Entering the anterior chamber
- Sudden aqueous drainage
- Rapid decompression of the globe
The surgeon may notice abrupt changes in ocular anatomy.
Delayed Postoperative SCH
Less commonly, hemorrhage develops hours or days after surgery.
Contributing factors include:
- Postoperative hypotony
- Valsalva maneuvers
- Excessive eye rubbing
- Trauma
- Sudden pressure fluctuations
Careful postoperative monitoring is therefore essential.
Clinical Signs During Surgery
Recognizing SCH early may prevent progression.
Warning signs include:
- Sudden shallowing of the anterior chamber
- Forward movement of the lens-iris diaphragm
- Increasing resistance during surgery
- Loss of red reflex
- Progressive globe firmness
- Difficulty maintaining chamber depth
Unexpected shallowing of the anterior chamber after decompression should immediately raise suspicion for SCH.
Postoperative Presentation
Children may present with:
- Sudden reduction in vision
- Ocular pain
- Red eye
- Elevated intraocular pressure
- Shallow anterior chamber
- Choroidal elevation on examination
Young children may instead demonstrate nonspecific symptoms such as irritability or reluctance to open the affected eye.
Diagnostic Evaluation
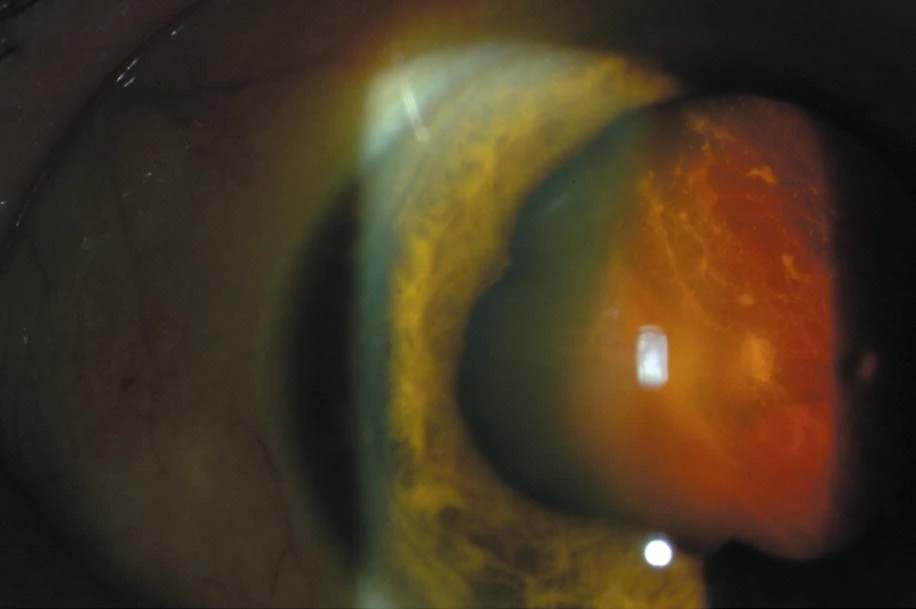
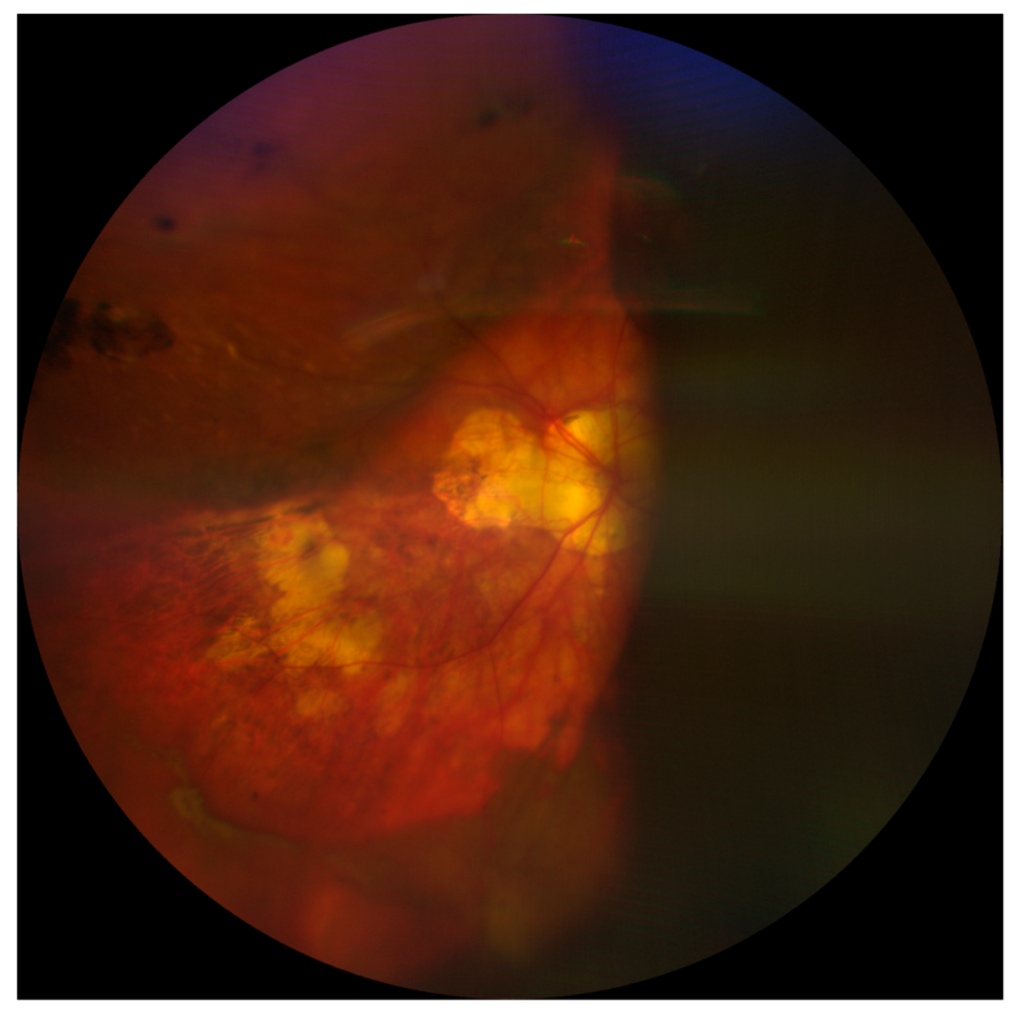
Clinical Examination
Fundus examination may reveal:
- Dark dome-shaped choroidal elevations
- Extensive choroidal detachment
- Vitreous hemorrhage in severe cases
Media opacity may limit visualization.
B-Scan Ultrasonography
B-scan remains the imaging modality of choice when posterior visualization is poor.
Typical findings include:
- Dome-shaped choroidal elevations
- Highly reflective suprachoroidal blood
- Appositional (“kissing”) choroidals
- Associated retinal detachment when present
B-scan is indispensable for confirming the diagnosis and monitoring resolution.
Optical Coherence Tomography
OCT has a limited role during acute massive hemorrhage but may later assist in evaluating:
- Macular involvement
- Secondary retinal changes
- Long-term structural recovery
Differential Diagnosis
Conditions that may mimic SCH include:
- Serous choroidal detachment
- Malignant glaucoma
- Retinal detachment
- Expulsive choroidal effusion
- Vitreous hemorrhage
Distinguishing these entities is important because management differs significantly.
Immediate Intraoperative Management
If SCH is suspected during surgery:
Initial Priorities
- Close all surgical incisions promptly
- Restore globe integrity
- Avoid further hypotony
- Maintain anterior chamber stability
Further manipulation should be minimized until the eye stabilizes.
Rapid wound closure is often the most important immediate intervention.
Postoperative Management
Treatment depends on the size and severity of the hemorrhage.
Conservative Management
Appropriate for:
- Small localized hemorrhages
- Stable intraocular pressure
- No retinal apposition
- Preserved visual potential
Management includes:
- Cycloplegics
- Corticosteroids
- Intraocular pressure control
- Close observation
Many limited hemorrhages gradually resolve without surgery.
Surgical Drainage
Drainage may be indicated when there is:
- Kissing choroidals
- Persistent apposition
- Uncontrolled IOP
- Retinal compromise
- Non-resolving massive hemorrhage
Drainage is generally delayed until clot liquefaction occurs, typically after 7–14 days, unless immediate intervention is required for severe complications.
Prevention Strategies
Preventing SCH begins before surgery.
Preoperative Measures
- Control markedly elevated IOP when possible
- Assess systemic bleeding risk
- Review coagulation status if indicated
Intraoperative Measures
- Avoid sudden ocular decompression
- Maintain anterior chamber depth
- Use viscoelastic strategically
- Control intraoperative hypotony
- Perform gentle tissue manipulation
Postoperative Measures
- Prevent hypotony
- Educate caregivers about avoiding eye rubbing
- Schedule close follow-up during the early postoperative period
Stable intraocular pressure throughout the perioperative period is the most effective preventive measure.
Prognosis
Visual outcomes vary widely depending on:
- Size of the hemorrhage
- Macular involvement
- Timing of diagnosis
- Associated retinal damage
- Underlying glaucoma severity
Small localized hemorrhages often resolve with favorable outcomes.
Massive SCH involving retinal apposition carries a significantly poorer prognosis despite appropriate management.
Future Perspectives
Although SCH remains rare in pediatric glaucoma surgery, advances in surgical technology may further reduce its incidence.
Areas of ongoing development include:
- Microincisional glaucoma surgery in selected pediatric cases
- Improved anterior chamber maintenance systems
- Intraoperative OCT guidance
- Enhanced viscoelastic materials
- Better perioperative risk stratification
Because pediatric SCH is uncommon, multicenter registries and collaborative studies will be essential for improving evidence-based management.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Papadopoulos M, Khaw PT. “Childhood glaucoma surgery.” Survey of Ophthalmology. 2007.
- Beck AD. “Diagnosis and management of pediatric glaucoma.” Ophthalmology Clinics of North America. 2001.
- Freedman SF, Jones SK. “Surgical management of primary congenital glaucoma.” Current Opinion in Ophthalmology. 2004.
- Chu TG, Green RL. “Suprachoroidal hemorrhage.” Survey of Ophthalmology. 1999.
- American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Glaucoma. Latest Edition.
- American Academy of Ophthalmology. BCSC: Pediatric Ophthalmology and Strabismus. Latest Edition.

{kind=link}