
Case Study
A 38-year-old woman presented with bilateral redness, blurred vision, and photophobia that had worsened over several weeks.


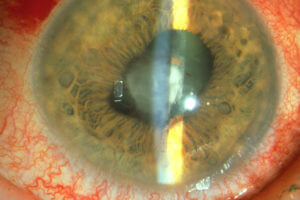
She reported a history of dry cough and fatigue but denied systemic symptoms such as fever or weight loss. On slit-lamp examination, she had mutton-fat keratic precipitates, anterior chamber cells, and posterior synechiae.
Fundoscopy revealed perivascular cuffing (“candle wax drippings”) and choroidal granulomas. A chest X-ray showed bilateral hilar lymphadenopathy, and serum angiotensin-converting enzyme (ACE) levels were elevated.
She was diagnosed with sarcoid uveitis and started on systemic corticosteroids and immunosuppressants, leading to symptom improvement.
Disease entity
Sarcoid uveitis is an inflammatory condition of the uveal tract associated with systemic sarcoidosis, a granulomatous disease of unknown etiology.
Sarcoid uveitis may manifest as anterior, intermediate, posterior, or panuveitis and is one of the most common ocular presentations of sarcoidosis.
While the exact pathogenesis remains unclear, immune dysregulation leading to granuloma formation is central. Early diagnosis and treatment are crucial to prevent vision-threatening complications.
Pathophysiology
Sarcoid uveitis arises from granulomatous inflammation triggered by an exaggerated immune response. Key mechanisms include:
- Granuloma Formation:
- T-cell-mediated immune response leads to the formation of non-caseating granulomas in the uveal tract.
- Cytokine Release:
- Elevated levels of tumor necrosis factor-alpha (TNF-α) and interleukins perpetuate inflammation.
- Vascular Involvement:
- Granulomatous inflammation around retinal vessels results in perivascular sheathing and ischemia.
Epidemiology
- Prevalence:
- Sarcoid uveitis accounts for approximately 10–15% of all uveitis cases.
- Demographics:
- Most commonly affects individuals aged 20–50 years.
- Higher prevalence in African American and Scandinavian populations.
- Gender Predilection:
- Slight female predominance.
Clinical Features
Sarcoid uveitis exhibits a wide spectrum of presentations depending on the anatomical location and severity of inflammation:
- Anterior Uveitis:
- Mutton-fat keratic precipitates.
- Iris nodules (Koeppe and Busacca nodules).
- Posterior synechiae.
- Intermediate Uveitis:
- Vitritis and snowballs in the vitreous cavity.
- Posterior Uveitis:
- Perivascular exudates (“candle wax drippings”).
- Choroidal granulomas.
- Retinal vasculitis and macular edema.
- Systemic Symptoms:
- Dry cough, dyspnea, fatigue, or skin lesions (erythema nodosum).
Examination Findings
- Slit-Lamp Examination:
- Granulomatous anterior chamber inflammation.
- Fundoscopy:
- Perivascular cuffing and granulomas.
- Vitreous haze in intermediate or posterior uveitis.
- Imaging:
- Chest X-ray or CT scan shows hilar lymphadenopathy.
- Fluorescein angiography highlights retinal vasculitis.

Differential Diagnosis
- Tuberculous uveitis.
- Vogt-Koyanagi-Harada (VKH) syndrome.
- Sympathetic ophthalmia.
- Syphilitic uveitis.
- Idiopathic uveitis.
Diagnosis
The diagnosis of sarcoid uveitis requires clinical and systemic evaluation. Key diagnostic tools include:
- Ocular Examination:
- Granulomatous features on slit-lamp and fundoscopic examination.
- Systemic Testing:
- Chest X-ray or high-resolution CT for hilar lymphadenopathy.
- Serum ACE levels (elevated in ~75% of cases).
- Lysozyme and calcium levels may also be elevated.
- Tissue Biopsy:
- Non-caseating granulomas from affected organs confirm the diagnosis.
Management
Treatment of sarcoid uveitis focuses on controlling inflammation and addressing systemic sarcoidosis:
- Corticosteroids:
- Topical corticosteroids for anterior uveitis.
- Systemic corticosteroids for intermediate, posterior, or panuveitis.
- Immunosuppressants:
- Methotrexate, azathioprine, or mycophenolate mofetil in refractory cases.
- Biologics:
- TNF-α inhibitors (e.g., infliximab) for severe or unresponsive cases.
- Adjunctive Treatments:
- Cycloplegic agents for pain relief in anterior uveitis.
- Anti-glaucoma medications if IOP is elevated.
Prognosis
With prompt treatment, sarcoid uveitis has a favorable visual prognosis. However, delayed diagnosis or inadequate treatment may lead to complications, including:
- Chronic glaucoma.
- Cataract formation.
- Macular edema and permanent vision loss.
Patients require long-term follow-up due to the relapsing-remitting nature of sarcoidosis.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Baughman, R. P., Lower, E. E., & du Bois, R. M. (2003). Sarcoidosis. Lancet, 361(9363), 1111–1118.
- James, W. E., & Tiedeman, J. S. (1989). Diagnosis and management of sarcoid uveitis. American Journal of Ophthalmology, 107(5), 559-567.
- Herbort, C. P., Rao, N. A., & Mochizuki, M. (2009). International criteria for the diagnosis of ocular sarcoidosis. Ocular Immunology and Inflammation, 17(3), 160–169.
- Iannuzzi, M. C., Rybicki, B. A., & Teirstein, A. S. (2007). Sarcoidosis. New England Journal of Medicine, 357(21), 2153–2165.
- Rosenbaum, J. T., & Pasadhika, S. (2013). Granulomatous uveitis: Challenges in diagnosis and management. Current Opinion in Rheumatology, 25(1), 1–8.

{kind=link}