
Case Study
A 24-year-old previously healthy woman presented with sudden, painless bilateral vision loss over one week. She reported mild photophobia and floaters but denied systemic symptoms such as fever or joint pain.


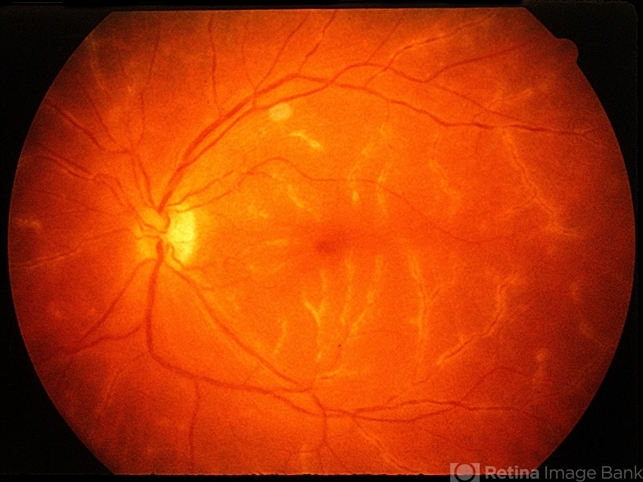
Ophthalmic examination revealed visual acuity of 20/80 in the right eye and 20/100 in the left eye. Fundus examination showed severe perivascular sheathing of retinal arteries and veins, giving a striking “frosted branch” appearance.
Fluorescein angiography confirmed extensive vascular leakage and optical coherence tomography (OCT) revealed macular edema.
Systemic workup, including infectious and autoimmune panels, was unremarkable. She was diagnosed with idiopathic frosted branch angiitis (FBA) and treated with systemic corticosteroids.
Over six weeks, her vision improved to 20/25 in both eyes, and the vascular sheathing resolved without recurrence.
Disease Entity
Frosted branch angiitis (FBA) is a rare inflammatory retinal vasculopathy characterized by severe perivascular sheathing of both arteries and veins.
The condition can be idiopathic or secondary to infectious, autoimmune, or neoplastic disorders. The name derives from the striking resemblance of the affected retinal vasculature to frost-covered tree branches.
Pathophysiology
The exact mechanism of FBA remains unclear, but the condition is believed to result from an inflammatory response leading to immune-mediated perivascular infiltration.
Possible underlying mechanisms include:
- Immune Dysregulation: Idiopathic cases may involve autoimmune attacks on retinal vessels, triggering widespread inflammation.
- Infectious Etiology: Some cases are linked to viral infections (e.g., Epstein-Barr virus, cytomegalovirus, herpes viruses), which can induce vasculitis.
- Paraneoplastic Association: Certain malignancies, such as leukemia and lymphoma, may trigger a secondary immune response affecting the retinal vasculature.
- Autoimmune Conditions: Systemic lupus erythematosus (SLE), Behçet’s disease, and sarcoidosis have been implicated in secondary FBA.

Epidemiology
- Age of Onset: Most cases occur in young adults, but the condition can affect individuals of any age.
- Sex Distribution: No clear gender predilection.
- Global Prevalence: Extremely rare, with only a few hundred cases reported in the literature.
Clinical Features
Symptoms
- Sudden-onset, painless vision loss (unilateral or bilateral)
- Floaters and photopsias
- Mild ocular discomfort or photophobia
- Occasionally, systemic symptoms if associated with infection or autoimmune disease
Fundoscopic Examination
- Marked, diffuse perivascular sheathing of retinal veins and arteries, resembling frost-covered tree branches
- Retinal hemorrhages (variable)
- Macular edema
- Vitritis (inflammatory cells in the vitreous) in some cases
Diagnostic Evaluation
Since FBA can be idiopathic or secondary, thorough ophthalmic and systemic evaluation is required.
Fundus Photography
- Documents the characteristic frosted branch appearance.
Fluorescein Angiography (FA)
- Diffuse vascular leakage from affected vessels.
- Delayed arteriovenous transit in severe cases.
Optical Coherence Tomography (OCT)
- Macular edema and retinal thickening.
- Hyperreflectivity along vessel walls due to inflammation.
OCT-Angiography (OCT-A)
- It may demonstrate capillary dropout or ischemia in severe cases.
Laboratory Workup
To rule out secondary causes, testing may include:
- Infectious Panel: Herpes viruses (HSV, VZV, CMV), HIV, syphilis, tuberculosis, toxoplasmosis.
- Autoimmune Workup: ANA, RF, ANCA, HLA-B51 (for Behçet’s disease).
- Oncology Screening: If malignancy is suspected (e.g., leukemia, lymphoma).
Differential Diagnosis
FBA must be distinguished from other retinal vascular diseases, including:
- Eales’ Disease: Affects young males and is associated with peripheral retinal nonperfusion.
- Behçet’s Uveitis: Recurrent hypopyon uveitis with retinal vasculitis.
- Sarcoid Vasculitis: Granulomatous inflammation with periphlebitis.
- Viral Retinitis (CMV, ARN, PORN): Typically associated with necrotizing retinitis.
Management
Treatment depends on whether the FBA is idiopathic or secondary to an underlying condition.
Corticosteroids
- Idiopathic Cases:
- High-dose oral corticosteroids (prednisone 1 mg/kg/day) tapered over several weeks.
- Intravenous methylprednisolone for severe cases.
- Autoimmune-Related Cases:
- May require long-term immunosuppression (e.g., methotrexate, mycophenolate mofetil).
Antiviral Therapy
- If viral etiology (e.g., herpes, CMV) is suspected, antiviral medications such as valganciclovir or acyclovir may be initiated.
Management of Secondary Causes
- Tuberculosis: Anti-tubercular therapy.
- Leukemia/Lymphoma: Oncologic treatment.
- Behçet’s Disease: Systemic immunosuppression.
Adjunctive Therapy
- Intravitreal Steroids: For persistent macular edema.
- Anti-VEGF Therapy: Rarely used but may help in refractory macular edema.
- Low Vision Aids: For patients with residual vision loss.
Prognosis
- Idiopathic Cases: Generally good prognosis with full recovery if treated promptly.
- Secondary Cases: Prognosis depends on the underlying condition; untreated systemic disease can lead to recurrence or chronic visual impairment.
- Complications:
- Retinal ischemia leads to neovascularization.
- Chronic macular edema causes permanent visual decline.
- Recurrence in cases with systemic autoimmune disease.

Conclusion
Frosted branch angiitis is a rare but visually striking retinal vasculitis that can present as an isolated ocular condition or a manifestation of systemic disease.
Prompt recognition and appropriate treatment, particularly with corticosteroids, can lead to good visual recovery.
Thorough systemic evaluation is essential to rule out secondary causes and guide management.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Kleiner RC, Kaplan HJ, Shakin JL, et al. Frosted branch angiitis: A clinical and fluorescein angiographic study. Ophthalmology. 1988;95(7):1025-1031.
- Walker S, Iguchi A, Jones NP. Frosted branch angiitis: A review. Eye (Lond). 2004;18(5):527-533.
- Lee MS, Gass JD. Frosted branch angiitis. Ophthalmology. 2002;109(4):713-722.
- Tappeiner C, Heinz C, Heiligenhaus A. Update on infectious uveitis and frosted branch angiitis. J Ophthalmic Inflamm Infect. 2012;2(2):61-68.
- Takeuchi M, Iwasaki T, Yoshikawa H, et al. Idiopathic frosted branch angiitis and its associated systemic diseases. Clin Exp Ophthalmol. 2017;45(1):62-68.

{kind=link}