
CASE REPORT
Case of Birdshot Retinochoroidopathy a 52-year-old female presented to a hospital complaining of “hundreds of floaters” that had been progressing for several months in both eyes. She noted a crescent shape to the floaters and one month of a small blurry spot in the inferonasal visual field in her right eye.

She also described nyctalopia, a less vivid quality to her vision, and morning photopsia and black spots upon awakening that lasted about 30 minutes.
Visual acuity was 20/20 in each eye and intraocular pressure by tonopen was 21 and 19 in the right and left eyes respectively. Her pupillary exam, visual fields, color vision, and motility were all normal.
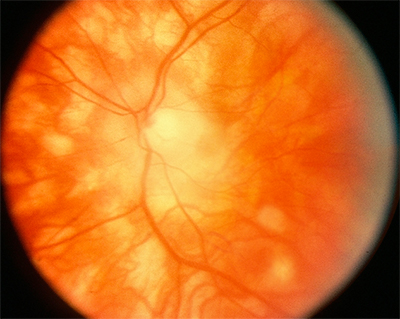
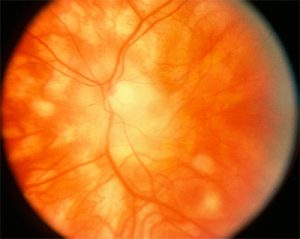
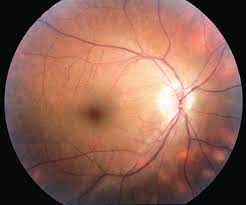
The Fundus exam revealed 1+ disc edema, bilateral epiretinal membranes, narrowing of her retinal vessels, and numerous mid-peripheral white/yellow choroidal spots bilaterally. ICG photos revealed areas of decreased dye perfusion within the choroid.
The differential diagnosis included inflammatory uveitis (birdshot chorioretinopathy, sarcoidosis), infectious causes (TB, syphilis, Lyme disease), and masquerade syndromes such as choroidal lymphoma. She was found to be HLA-A29 positive.
An extensive laboratory work-up was otherwise negative. Full-field electroretinograms showed attenuated scotopic dim blue flash ERGs to about 59% with a slowed photopic b-wave time of 35 milliseconds.
The patient was diagnosed with Birdshot Chorioretinopathy (BSCR).
DISEASE of Birdshot Retinochoroidopathy
Birdshot Retinochoroidopathy (BSRC) is a distinct type of posterior uveitis. Its characteristics include minimal anterior segment inflammation and diffuse posterior choroidopathy with vitritis and retinal vasculitis. The precise etiology of this disease is yet to be elucidated.

various treatment modalities have been employed with the ultimate goal of durable remission of this vision-threatening intraocular disease.

MANAGEMENT of Birdshot Retinochoroidopathy
Long-term monotherapy with corticosteroids is inadequate to induce durable remission in BSRC. The efficacy of regional steroid injections is transient and limited to treating acute inflammatory exacerbations and macular edema.
Early administration of immunomodulatory agents is recommended to prevent disease progression and vision-threatening complications.
A variety of immunosuppressive agents, including cyclosporine, methotrexate, azathioprine, derivatives of mycophenolic acid, intravenous immunoglobulin, anti-tumor necrosis factor-alpha (Anti-TNF α) inhibitors, and daclizumab have been administered as monotherapy or as combination therapy in the treatment of BSRC.
CONCLUSION
Birdshot Retinochoroidopathy is an autoimmune inflammatory disease restricted to the eye, with a strong association with the HLA-A29 gene. It is also associated with elevated systemic levels of IL-17, IL-21, IL-23, and TGF-β1, highlighting the systemic involvement of the disease and hence the importance of systemic therapy.
Administering traditional immunosuppressive agents such as cyclosporine and mycophenolate mofetil to accomplish 2-year steroid-free remission, and then slowly tapering to completion, has shown encouraging results for adequate treatment of Birdshot Retinochoroidopathy (BSRC).
Biologics are considered for uveitis refractory to traditional IMT. Appropriate treatment and rigorous monitoring for this sight-threatening disease can achieve remission and, in many cases, a cure.
would you have the interest to take retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera.

More: Macroaneurysms, Arlt’s Triangle, Crocodile Shagreen, Morgagnian Cataract, Cogan’s syndrome
REFERENCES
- Franceschetti A, Babel J. La chorio-rétinite en taches de bougie, manifestation de la maladie de Besnier-Boeck. Ophthalmologica. 1949;118(4-5):701-10.
- Ryan SJ, Maumenee AE. Birdshot retinochoroidopathy. Am J Ophthalmol. 1980;89(1): 31-45.
- Kaplan HJ, Aaberg TM. Birdshot retinochoroidopathy. Am J Ophthalmol. 1980;90(6): 773-82.
- Gass JD. Vitiliginous chorioretinitis. Arch Ophthalmol. 1981;99(10):1778-87.
- Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D’Amico DJ, et al. Referral patterns of uveitis in a tertiary eye care center. Arch Ophthalmol. 1996; 114(5):593-9. Comment in: Arch Ophthalmol. 1996;114(5):604-5; Arch Ophthalmol. 1997; 115(4):565-6.
- Levinson RD, Brezin A, Rothova A, Accorinti M, Holland GN. Research criteria for the diagnosis of birdshot chorioretinopathy: results of an international consensus conference. Am J Ophthalmol. 2006;141(1):185-7.

{kind=link}