
Disease
Central foveal bouquet abnormalities are described on optical coherence tomography (OCT) in vitreomacular interface disorders and cystoid macular edema (CME).

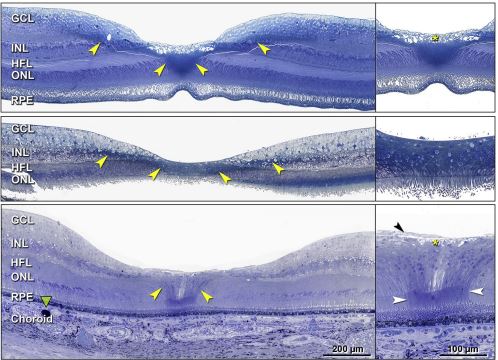
They comprise alterations within the central bouquet (CB), defined as a small circular area in the central fovea, approximately 100 microns and composed of cone photoreceptors and Muller cells. They represent a continuous clinical spectrum based on progressive morphological appearances.
These include :
- Stage 1- Cotton ball sign
- Stage 2- Foveolar detachment
- Stage 3- Acquired vitelliform lesion.
Etiology
- CB abnormalities are noted in association with vitreomacular interface disorders. These have been often reported in eyes with epiretinal membrane (ERM). Apart from these, they have also been observed in non-tractional macular conditions such as CME.
Diagnosis
Diagnosis of CB abnormalities is made based on OCT findings.
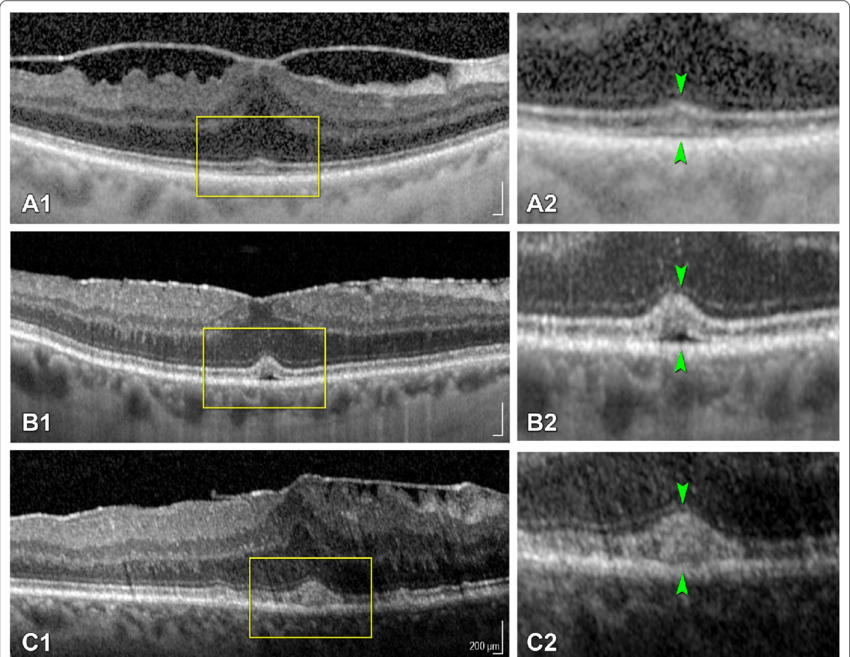
- Stage 1 (cotton ball sign) is characterized by a small, fuzzy subfoveal hyperreflective area between the inner segment ellipsoid zone (EZ) and the interdigitation zone (IZ).
- In stage 2 (foveolar detachment), there is a central subfoveal hyporeflective pocket corresponding to subretinal fluid accumulation under the interdigitation zone.
- In stage 3 (acquired vitelliform lesion), there is the presence of thick dome-shaped subfoveal hyperreflective material between the ellipsoid zone and retinal pigment epithelium.
- Additionally, OCT can also demonstrate findings related to vitreomacular interface disorders. In eyes having ERM, OCT will show ERM as a hyperreflective line above ILM along with intraretinal findings specific to the stages of ERM. These may include foveal herniation and ectopic inner foveal layers (EIFL).
- EIFL has been observed in stage 3 and 4 ERM and was found to be associated with a lower incidence of CB abnormalities. This has been attributed to EIFL causing reduced displacement and stretching of the outer retina at the fovea.
Symptoms
- Symptoms are related to the underlying macular pathologies and may include blurred vision and metamorphopsia.
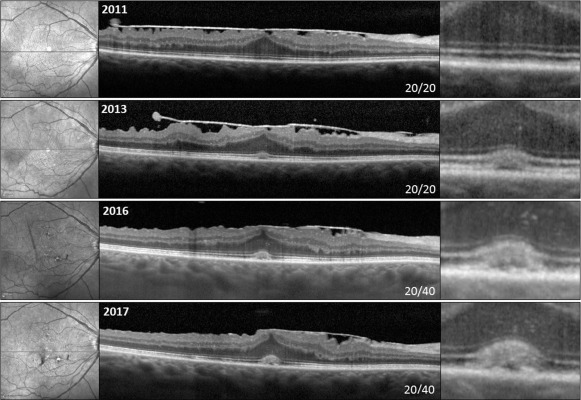
- Previous studies have observed a correlation between stages of CB abnormalities and visual acuity.
- Govetto et al. studied CB abnormalities in eyes with ERM and observed that visual acuity was better in the presence of cotton ball signs and worsened with progression to subsequent stages. This may be related to EZ disruption seen in advanced stages of CB abnormalities.
- In eyes with CME, the presence of CB abnormalities was found to be associated with increased macular thickness, horizontal extent of edema, and worse visual acuity at baseline.
Differential diagnosis
CB abnormalities need to be differentiated from conditions such as:
- Acute retinal pigment epitheliitis (Krill disease) – It has an acute onset with painless loss of vision or central scotoma. OCT shows a dome-shaped hyperreflective lesion at the level of the photoreceptors layer disrupting the ellipsoid zone and interdigitation zone. There may be initial involvement of the outer nuclear layer. The disease is known to have rapid resolution in 6 to 12 weeks.
- Central serous chorioretinopathy – The patient usually presents with complaints of unilateral central vision loss with or without distortion or a possible central scotoma. However, the presentation can be bilateral. CSCR is usually self-limiting and resolves spontaneously within 2 to 3 months. However, recurrent episodes are known to occur. OCT may show serous PED, hyper-reflective, fibrinous sub-retinal fluid, RPE defect corresponding to potential leakage site, and choroidal thickening.
- Best Disease and Bestrophinopathies – Best vitelliform macular dystrophy generally presents the first decade of life and is usually bilateral. Early stages are associated with minimal visual symptoms. Progression of stages is associated with a gradual decrease in visual acuity. Adult-onset foveomacular vitelliform dystrophy is typically seen between 30-50 years of age with minimal visual symptoms. OCT may show nonhomogenous hyperreflectivity at the level of RPE and thickening of the cone’s outer segments. OCT can also pick up the development of CNV in the later stage.
- Solar retinopathy – The patient has a history of direct sun-gazing or eclipse viewing. Usually, there is bilateral foveal involvement with OCT showing disruption of the outer retinal layers.
- Acute idiopathic maculopathy – The patient presents with acute unilateral visual loss. OCT shows subfoveal hyperreflective thickening at the level of the outer retina and RPE and hyporeflective fluid in subretinal space. It is generally a self-limiting condition.
Management
- Management includes treatment of underlying associations. These include treating ERM and CME due to various etiologies.
- While CME can be treated with topical non-steroidal anti-inflammatory (NSAID) eyedrops / intravitreal injections / oral therapy, ERM needs pars plana vitrectomy (PPV) for removal.
References
- Govetto A, Bhavsar KV, Virgili G, Gerber MJ, Freund KB, Curcio CA, et al. Tractional Abnormalities of the Central Foveal Bouquet in Epiretinal Membranes: Clinical Spectrum and Pathophysiological Perspectives. Am J Ophthalmol. 2017;184:167-180.
- Tsunoda K, Watanabe K, Akiyama K, Usui T, Noda T. Highly reflective foveal region in optical coherence tomography in eyes with vitreomacular traction or epiretinal membrane. Ophthalmology 2012;119:581–587.
- Pison A, Dupas B, Couturier A, Rothschild PR, Tadayoni R. Evolution of subfoveal detachments secondary to idiopathic epiretinal membranes after surgery. Ophthalmology 2016; 123:583–589.
- Dupas B, Tadayoni R, Erginay A, et al. Subfoveal deposits secondary to idiopathic epiretinal membranes. Ophthalmology 2009;116:1794–1798.
- Brinkmann MP, Michels S, Brinkmann C, Rommel F, Ranjbar M, Graf Johansen N, Becker M. Epiretinal membrane surgery outcome in eyes with abnormalities of the central bouquet. Int J Retina Vitreous. 2021;7:7.

{kind=link}