
CASE REPORT
A 19 years old male presented with a 4-day history of bilateral central scotoma following 10-15 minutes of direct sun-gazing during the solar eclipse. On general examination, he was of normal build and height for his age.

Upon ocular examination, his BCVA was 6/9 in both eyes. Slit-lamp microscopic examination showed clear cornea in both eyes. Pupils of both eyes were round, regular, and reacting. Lens was clear in both eyes.
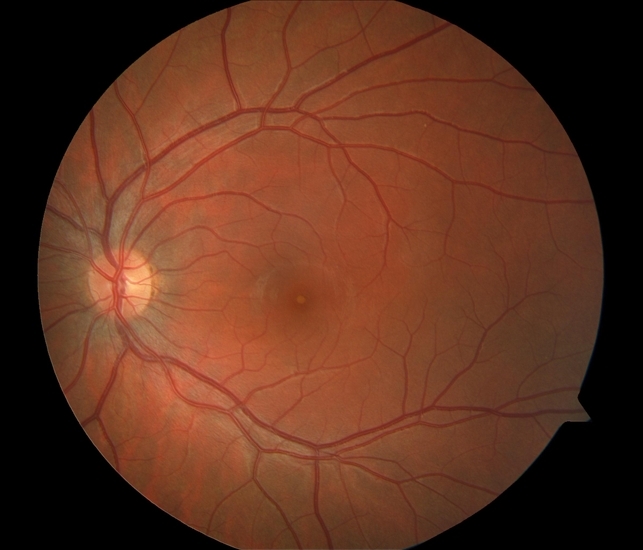
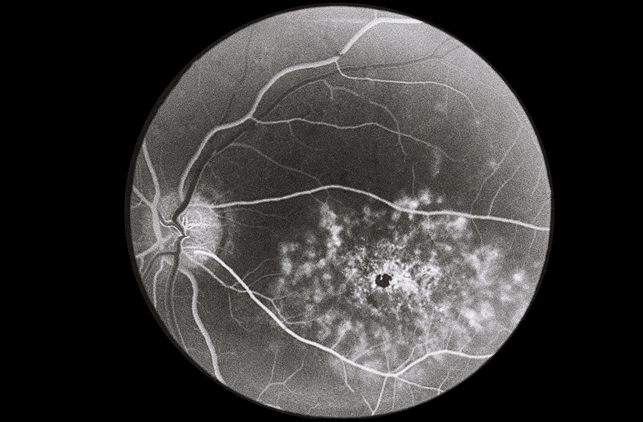
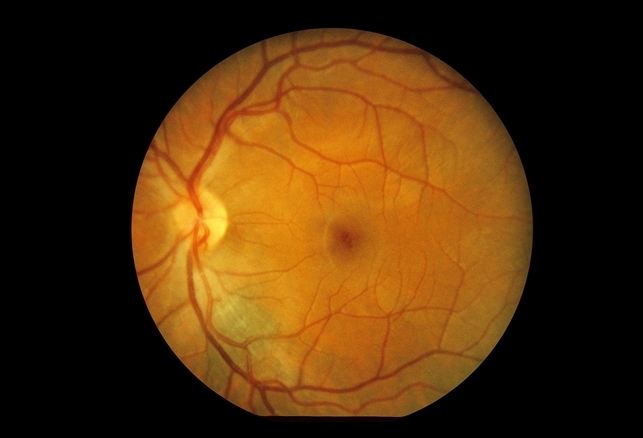
Fundus examination revealed discrete yellow lesions at the fovea of both eyes. Optical coherence tomography (OCT) scanning showed corresponding retinal pigment epithelial defects in both eyes.
Based on the clinical and OCT findings, a diagnosis of solar eclipse-induced retinopathy was confirmed.
solar retinopathy DISEASE entity
Solar retinopathy (also known as, photic retinopathy, foveomacular retinitis, solar retinitis, and eclipse retinopathy) refers to photochemical toxicity and resultant injury to retinal tissues, usually occurring at the fovea.
This entity is commonly associated with sungazing or eclipse viewing and often results in mild-to-moderate visual acuity deficit and/or central or paracentral scotomata.
Recovery is spontaneous in nature and occurs over the course of 3-6 months after the inciting event, though visual recovery may be incomplete and the patient may suffer from permanent visual acuity deficits and central or paracentral scotomata.
solar retinopathy MANAGEMENT
No known beneficial treatment exists for solar retinopathy, although entities such as steroids have been tried without consistent evidence of effectiveness. Prevention through education is paramount.
Prognosis
The bulk of visual acuity improvement has been noted to take place in the first 1 and 6 months after the phototoxic event. Despite more moderate vision loss at presentation, most patients ultimately return to a visual acuity level of 20/20-20/40.
Improvement has been shown to be achieved earlier and more robustly in patients with visual acuity of 0.2 logMAR (20/30 Snellen visual acuity) at presentation. Furthermore, a correlation was found between initial visual acuity and fundoscopic appearance 2 weeks after the phototoxic event.
Unfortunately, metamorphopsia and central or paracentral scotomata, including those that show some improvement initially, may become permanent.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Yannuzi LA, Fisher YL, KruegerA, et al. Solar Retinopathy: A photobiological and geophysical analysis. Tr. Am. Ophth Soc. 1987; 85:120-158.
- Michels M, Sternberg P, Operating microscope-induced retinal phototoxicity: pathophysiology, clinical manifestations and prevention. Surv Ophthalmol. 1990; 34:237-252.
- Long VW, Woodruff GH. Bilateral retinal phototoxic injury during cataract surgery in a child. J AAPOS. 2004; 8(3):278-9.
- Yang C, Shao D, Ding X, et al. Chronic phototoxic maculopathy caused by welding arc in occupational welders. Can J Ophthalmol. 2012; 47(1):45-50.
- Michels M, Lewis H, Abrams GW, et al. Macular phototoxicity caused by fiberoptic end illumination during pars plana vitrectomy. Am J Ophthalmol. 1992; 114(3):287-96.
- Robertson DM, Lim TH, Salomao DR, et al. Laser pointers and the human eye: a clinicopathologic study. Arch Ophthalmol. 2000; 118(12):1687-1691.
- Tarigopula S, Chod R. Unpublished Case. St. Louis University Eye Institute. St. Louis University, St. Louis, MO.

{kind=link}