
Case Study
A 32-year-old male presented with gradual blurring of vision and floaters in his left eye over several months. He denied pain or redness.


Family history was notable for renal tumors in a first-degree relative. Best-corrected visual acuity was 20/20 in the right eye and 20/40 in the left eye.
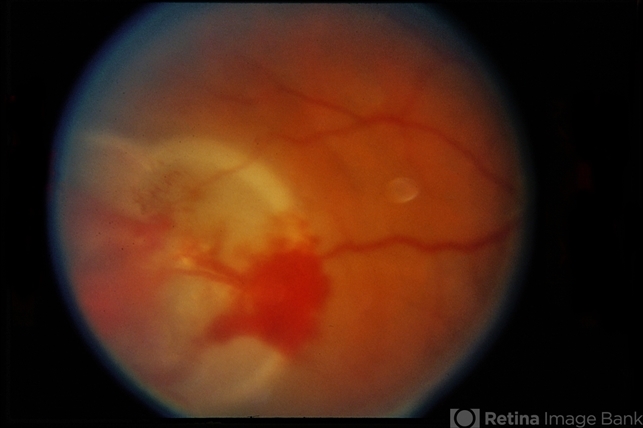
Fundus examination of the left eye revealed a well-circumscribed, reddish-orange vascular mass in the superotemporal peripheral retina, supplied by a dilated tortuous feeder arteriole and drained by an enlarged vein.
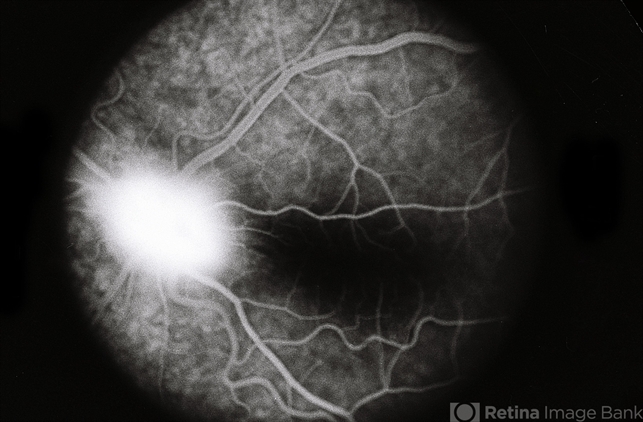
Surrounding lipid exudation and localized serous retinal detachment were noted. Fluorescein angiography showed early hyperfluorescence with intense late leakage.
A diagnosis of retinal capillary hemangioblastoma was made, and systemic evaluation was initiated to exclude von Hippel–Lindau disease.
Disease Entity
Retinal capillary hemangioblastoma (RCH), also known as retinal hemangioblastoma or retinal angioma, is a benign but potentially vision-threatening vascular tumor of the retina.
It is composed of proliferating capillary-sized blood vessels and stromal cells. These tumors may occur sporadically or as part of von Hippel–Lindau (VHL) disease, an autosomal dominant multisystem disorder.
Although histologically benign, retinal capillary hemangioblastomas can lead to significant visual morbidity due to exudation, retinal detachment, vitreous hemorrhage, and secondary glaucoma if left untreated.
Pathophysiology
The tumor arises from abnormal proliferation of retinal capillaries, leading to the formation of a vascular mass with high permeability. Leakage of plasma lipids and fluid from these vessels results in:
-
Intraretinal and subretinal exudation
-
Macular edema
-
Serous or tractional retinal detachment
In VHL-associated cases, mutations in the VHL tumor suppressor gene lead to increased hypoxia-inducible factors (HIFs), promoting angiogenesis through upregulation of vascular endothelial growth factor (VEGF).
Etiology and Classification
Retinal capillary hemangioblastomas are classified into:
Sporadic
-
Usually solitary
-
Often diagnosed later in life
-
Less likely to have bilateral or multiple lesions
VHL-Associated
-
Frequently multiple and bilateral
-
Occur at a younger age
-
Associated with systemic tumors such as cerebellar hemangioblastomas, renal cell carcinoma, pheochromocytoma, and pancreatic cysts
Epidemiology
-
Typically diagnosed in the second to fourth decades of life
-
No strong gender predilection
-
Up to 60% of patients with retinal capillary hemangioblastoma have underlying VHL disease
-
Retinal involvement is often the earliest manifestation of VHL
Clinical Features
Symptoms depend on tumor size, location, and secondary complications.
Common presentations include:
-
Blurred or decreased vision
-
Floaters
-
Metamorphopsia
-
Visual field defects
Peripheral tumors may remain asymptomatic until significant exudation occurs, while juxtapapillary lesions can cause early visual loss.
Examination Findings
Fundus Examination
-
Round or oval, orange-red vascular mass
-
Prominent dilated feeder artery and draining vein
-
Surrounding lipid exudation
-
Localized or extensive serous retinal detachment
Imaging
-
Fluorescein angiography: Early hyperfluorescence with progressive leakage
-
OCT: Macular edema, subretinal fluid, and exudates
-
B-scan ultrasonography: Elevated retinal lesion with high internal reflectivity (for larger tumors)
Wide-field imaging is useful for detecting peripheral and multiple lesions.
Differential Diagnosis
-
Coats disease
-
Retinal vasoproliferative tumor
-
Choroidal hemangioma
-
Cavernous hemangioma of the retina
-
Inflammatory or neoplastic retinal masses
The presence of dilated feeder vessels is a key distinguishing feature.
Diagnosis
Diagnosis is primarily clinical, supported by angiographic findings. In all patients—especially young individuals or those with multiple or bilateral tumors—systemic evaluation for VHL disease is mandatory, including:
-
Neuroimaging
-
Abdominal imaging
-
Genetic testing when appropriate
Management
Treatment depends on tumor size, location, activity, and associated complications.
Observation
-
Small, inactive tumors without exudation
-
Close monitoring is essential
Local Therapies
-
Laser photocoagulation: Effective for small peripheral lesions
-
Cryotherapy: Preferred for larger peripheral tumors with subretinal fluid
-
Photodynamic therapy: Useful in selected cases
Adjunctive Treatments
-
Intravitreal anti-VEGF injections may reduce exudation but are rarely sufficient as monotherapy
Surgical Management
-
Pars plana vitrectomy may be required for:
-
Non-resolving retinal detachment
-
Vitreous hemorrhage
-
Epiretinal membrane formation
-
Prognosis
Visual prognosis depends on:
-
Tumor location (macular or juxtapapillary lesions have worse outcomes)
-
Degree of exudation and retinal detachment
-
Timeliness of treatment
Early detection and treatment can preserve good visual function, particularly in peripheral tumors.
Follow-Up and Systemic Implications
Patients require long-term ophthalmic follow-up due to the risk of:
-
Tumor recurrence
-
Development of new lesions
-
Progressive exudative complications
In VHL-associated cases, lifelong systemic surveillance is critical.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Shields JA, Shields CL. Vascular tumors of the retina and optic disc. Ophthalmology.
-
Singh AD, Shields CL, Shields JA. Von Hippel–Lindau disease. Surv Ophthalmol.
-
American Academy of Ophthalmology. Basic and Clinical Science Course: Retina and Vitreous.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier.
-
Tasman W, Jaeger EA. Duane’s Ophthalmology. Lippincott Williams & Wilkins.

{kind=link}