
Case Presentation
A 28-year-old male presented to the emergency department with sudden vision loss in the right eye following a high-velocity pellet gun injury to the left orbit two hours prior.


He reported no prior ocular history or systemic comorbidities but endorsed immediate blurry vision and floaters in the affected eye.
On examination, best-corrected visual acuity measured counting fingers at 2 feet in the right eye and 20/20 in the left.
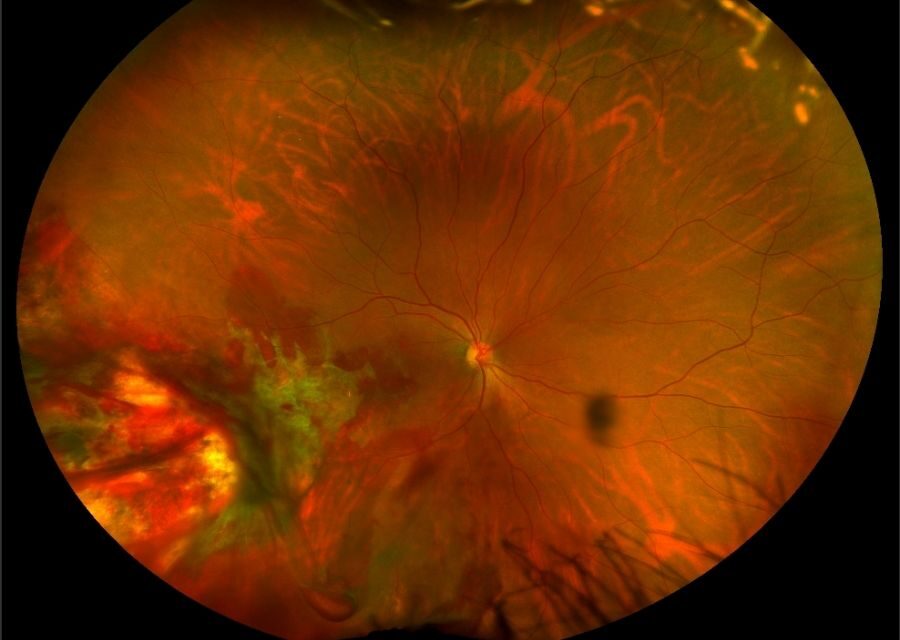
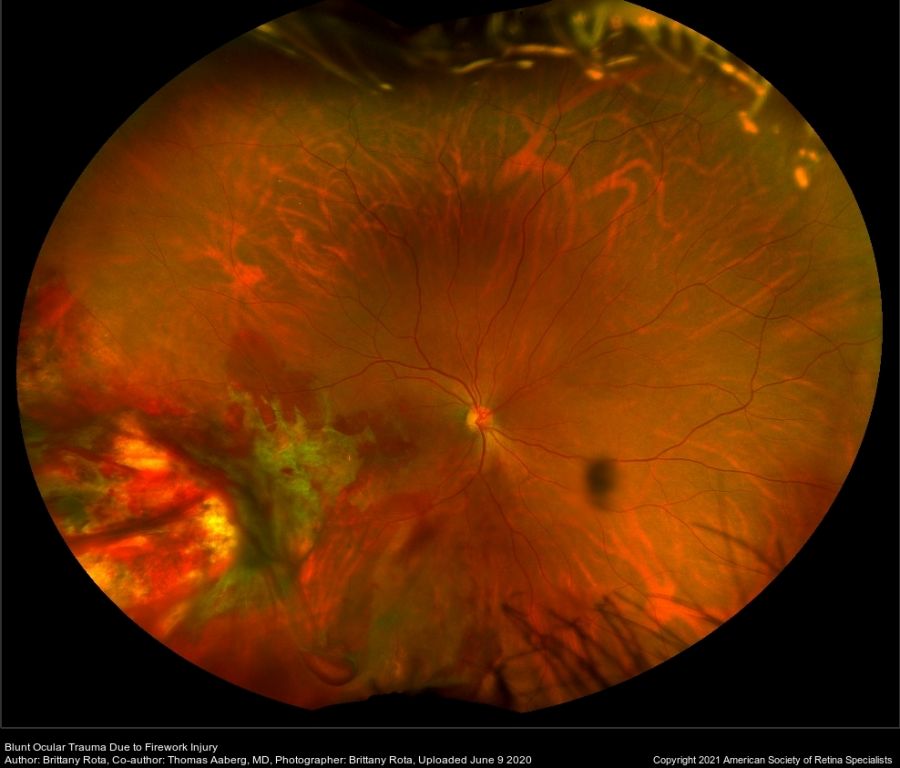
Slit-lamp evaluation revealed a clear anterior segment with 1+ vitreous cells. Dilated fundus exam showed inferotemporal bare sclera with surrounding chorioretinal rupture, intraretinal hemorrhage, and dense vitreous hemorrhage precluding macular detail.
B-scan ultrasonography confirmed an intact globe with layered posterior vitreous hemorrhage. A diagnosis of Retinitis Sclopetaria was made.
Disease Overview
Retinitis Sclopetaria represents a full-thickness rupture of the choroid and neurosensory retina caused by indirect high-velocity trauma to the closed globe.
Ophthalmologists encounter this rare entity in trauma settings, often from projectiles like bullets or BB pellets passing adjacent to the eye.
The condition demands prompt recognition because it spares the sclera yet inflicts profound posterior segment damage.
Clinicians must differentiate it from other blunt traumas to guide management.
Its importance lies in the potential for vision-threatening complications like vitreous hemorrhage progression or retinal detachment, despite fibroglial scarring that often stabilizes the retina.
Early intervention prevents secondary issues, preserving maximal visual potential in young patients.
Pathophysiology
High-velocity projectiles generate shock waves that deform the globe without penetrating it. These forces exploit tissue elasticity differences. The inelastic Bruch membrane ruptures first under compressive stress.
Choriocapillaris attached to Bruch membrane tears, causing acute subretinal hemorrhage. The retinal pigment epithelium, also rigid, disrupts alongside.
Elastic neurosensory retina and sclera withstand initial impact but split and retract.
Direct coup injury occurs at the impact site, exposing bare sclera. Contrecoup effects may add remote damage like commotio retinae. Vitreous hemorrhage follows from vascular disruption.
Histopathology reveals photoreceptor loss, choroidal defects, and retinal pigment epithelium hyperplasia. Loose fibrous tissue initially replaces the rupture site. Dense connective tissue forms scars over weeks.
Fibroglial proliferation fuses retina to choroid, reducing detachment risk. Inflammatory mediators drive this repair. Persistent hemorrhage risks organization into tractional elements.
Epidemiology
Retinitis Sclopetaria predominantly affects young adults in their second to fourth decades. Victims often engage in high-risk activities involving firearms or projectiles.
Males outnumber females by a ratio exceeding 5:1, reflecting exposure patterns in trauma demographics. Urban violence and recreational shooting contribute to cases.
Key risk factors include proximity to high-velocity objects like bullets, BB guns, or blasts. Orbital foreign bodies amplify shock wave transmission. No genetic predisposition exists; incidence rises with civilian gunfire reports over recent decades.
Clinical Features
- Patients report acute vision loss, often counting fingers or worse, due to hemorrhage obscuring the visual axis.
- Floaters and photopsia arise from vitreous hemorrhage and retinal disruption.
- Onset is immediate post-trauma, with progression over days as the hemorrhage organizes.
- Blurred vision persists if macular involvement occurs.
- Relative afferent pupillary defect develops in severe cases.
- Extraocular motility deficits signal orbital involvement.
- Unilateral presentation dominates; bilateral rare unless there is multisite trauma.
- Pain is minimal unless concurrent anterior injury.
Examination Findings
- Visual acuity ranges from no light perception to 20/200, depending on hemorrhage density and macular status.
- Anterior segment typically normal; mild vitreous cells possible.
- Fundus shows bare sclera at the rupture site with chorioretinal tears, often quadrantic
- Vitreous, intraretinal, and subretinal hemorrhages layer posteriorly.
- Optic disc edema and retinal whitening (commotio) are common acutely.
- OCT reveals full-thickness defects, choroidal excavation, and outer retinal disruption.
- Fluorescein angiography demonstrates hypofluorescence at rupture with late staining.
- Ultrawide-field imaging captures peripheral bare sclera and fibrotic evolution.
- B-scan confirms intact globe and hemorrhage layering.
Differential Diagnosis
- Choroidal rupture: Lacks bare sclera; often contrecoup.
- Commotio retinae: Superficial whitening without full-thickness tear.
- Traumatic retinal detachment: Involves retinal breaks beyond the rupture site.
- Vitreous hemorrhage from other trauma: No chorioretinal defect.
- Berlin edema: Diffuse whitening without rupture.
- Orbital foreign body with secondary effects: Imaging differentiates.
- Endophthalmitis: Inflammatory signs predominate.
Diagnosis
Clinicians diagnose Retinitis Sclopetaria through detailed trauma history and dilated fundus examination. Bare sclera with adjacent chorioretinal rupture confirms the entity.
Imaging supports but does not supplant clinical findings. B-scan ultrasonography rules out globe rupture and assesses hemorrhage. OCT delineates layer-specific defects. Fluorescein angiography highlights nonperfusion.
Ancillary tests include orbital CT to exclude foreign bodies. Gonioscopy checks angle recession. Serial exams monitor evolution. No laboratory tests prove diagnostic.
Management
Observation
The primary approach favors close observation in uncomplicated cases. Fibroglial scarring naturally adheres the retina to the choroid. Monitor weekly initially for hemorrhage clearance and detachment.
Medical Treatment
Administer topical corticosteroids like prednisolone acetate 1% hourly to curb inflammation. Cycloplegics such as scopolamine aid comfort.
Taper steroids over weeks. Antiglaucoma agents control rare pressure spikes. Systemic steroids are reserved for optic neuropathy.
Surgical Treatment
Reserve pars plana vitrectomy for non-clearing vitreous hemorrhage or rhegmatogenous detachment. Scleral buckling addresses remote breaks.
Evidence shows no visual benefit from early surgery versus observation. Intervene if vision threatens or complications arise. Orbital exploration precedes if a foreign body is suspected.

Prognosis
Visual outcomes vary widely; most achieve 20/200 or worse due to macular scarring. Improvement occurs in two-thirds as hemorrhage resorbs, reaching 20/60 in select cases.
Favorable factors include foveal sparing, minimal macular hemorrhage, and young age with vitreous adherence. Poor predictors encompass central involvement, optic neuropathy, and delayed detachment.
Follow-up entails monthly dilated exams for six months, then quarterly. Surveillance detects late detachment (11% risk) or neovascularization. Polycarbonate lenses prevent recurrence.
Prevention
Counsel patients on firearm safety and protective eyewear during shooting sports. Remove orbital foreign bodies promptly to avert shock wave transmission.
No screening exists for at-risk populations. Educate trauma teams on recognition. Public health measures reduce projectile violence.
References
1. American Academy of Ophthalmology. Chorioretinitis Sclopetaria. EyeWiki.
2. Choroida Education. Chorioretinitis Sclopetaria: Case Study, Diagnosis and Management. 2022.
3. University of Iowa. Chorioretinitis Sclopetaria: A Systems Based Approach. Eye Forum.
4. PubMed. Treatment and Pathogenesis of Traumatic Chorioretinal Rupture (Sclopetaria). 1994.
5. Retina Today. Bullet Proof: A Case of Chorioretinitis Sclopetaria. 2024.

{kind=link}