
Case Study
A 59-year-old man presented to an ophthalmology clinic with sudden, painless vision loss in his right eye upon awakening that morning.

He described a “shadow” in the lower half of his visual field and difficulty reading with the affected eye. He denied headache, scalp tenderness, jaw claudication, or systemic symptoms.

Past medical history included poorly controlled type 2 diabetes mellitus, systemic hypertension, and hyperlipidemia.
He was a non-smoker but had been recently experiencing increased stress and irregular sleep due to work demands. There was no history of recent eye trauma or ocular surgery.
On examination, his best-corrected visual acuity was 6/18 in the right eye and 6/6 in the left eye. Relative afferent pupillary defect (RAPD) was present on the right.
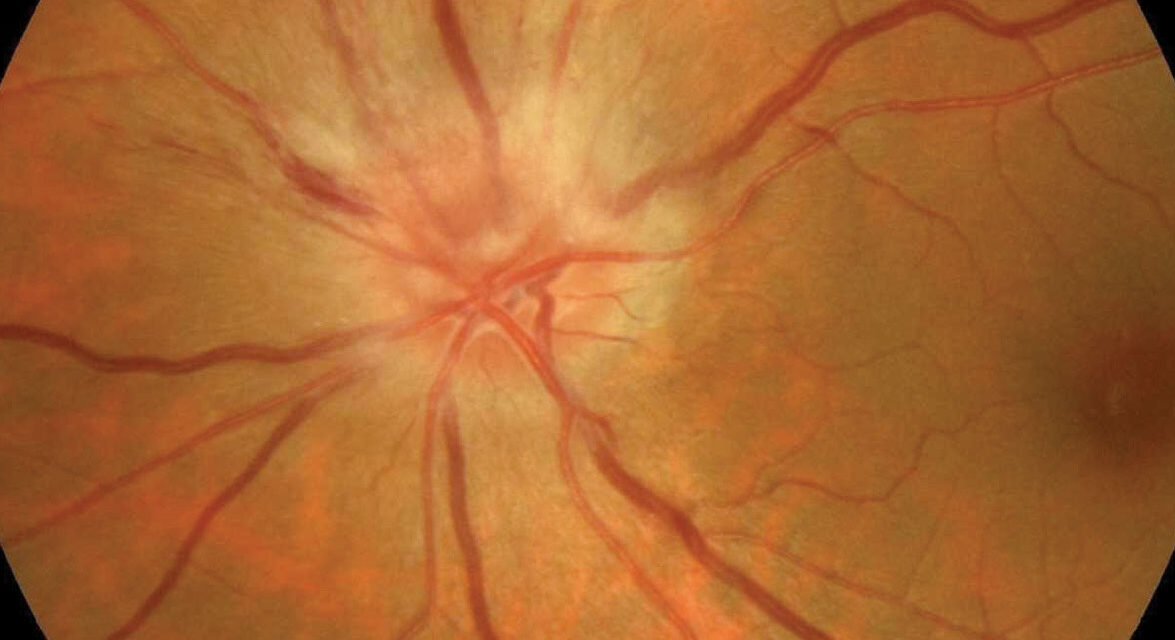
Confrontation visual field testing revealed an inferior altitudinal defect. Fundus examination of the right eye showed a swollen, pale optic disc with blurred margins and peripapillary splinter hemorrhages.
The left optic disc was noted to have a small, crowded appearance (“disc at risk”) without swelling.
Optical coherence tomography (OCT) confirmed optic disc edema in the right eye with preserved retinal layers, and fluorescein angiography revealed delayed filling of the optic disc without evidence of choroidal hypoperfusion.
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels were within normal limits, effectively ruling out arteritic causes such as giant cell arteritis.
The final diagnosis was non-arteritic anterior ischemic optic neuropathy (NAION) in the right eye, likely precipitated by nocturnal hypotension in the setting of vascular risk factors.
Introduction
Non-Arteritic Anterior Ischemic Optic Neuropathy (NAION) is the most common acute optic neuropathy in individuals over the age of 50.
It results from infarction of the optic nerve head due to insufficient perfusion of the short posterior ciliary arteries, without an inflammatory or arteritic component.
Unlike arteritic AION (most often caused by giant cell arteritis), NAION typically presents as sudden, painless vision loss upon awakening and is strongly associated with systemic vascular risk factors.
The condition is often precipitated by nocturnal hypotension or other events that compromise optic nerve head perfusion, particularly in patients with “crowded” optic discs, known as the disc at risk.
While the exact pathogenesis remains multifactorial, the disease represents a significant cause of irreversible visual impairment in the middle-aged and elderly population.
Pathophysiology
NAION occurs due to insufficient blood flow in the prelaminar portion of the optic nerve head supplied by the short posterior ciliary arteries.
In susceptible individuals with a structurally small optic disc, the swollen nerve fibers have limited room to expand, leading to compartment-like compression and further vascular compromise — a “vicious cycle” of ischemia and swelling.
The primary mechanism involves:
-
Nocturnal hypotension reduces optic nerve perfusion during sleep.
-
Atherosclerosis or microvascular disease impairs autoregulation of optic nerve blood flow.
-
Disc crowding increases susceptibility to ischemic damage.
Pathologic findings include axonal swelling, secondary ganglion cell loss, and gliosis. Importantly, the process is non-inflammatory, differentiating it from arteritic causes.
Epidemiology
-
Age group: It typically affects individuals over 50 years.
-
Gender: Slight male predominance in some studies, but not universally observed.
-
Incidence: Estimated at 2–10 per 100,000 population annually.
-
Risk factors:
-
Systemic hypertension
-
Diabetes mellitus
-
Hyperlipidemia
-
Sleep apnea
-
Smoking
-
Nocturnal hypotension (often due to antihypertensive medication timing)
-
Small, crowded optic discs (disc at risk)
-
Clinical Features
-
Onset: Sudden, painless vision loss, often noticed on awakening.
-
Severity: Variable; may range from mild blurring to profound loss.
-
Visual field defects: Classically altitudinal (inferior > superior).
-
Color vision: Often reduced in proportion to acuity loss.
-
Relative afferent pupillary defect: Present in unilateral or asymmetric cases.

Examination Findings
-
Fundoscopy:
-
Swollen, pale optic disc with indistinct margins.
-
Peripapillary hemorrhages.
-
Sectoral or diffuse disc edema.
-
-
Contralateral eye:
-
May reveal small, crowded optic disc (predisposing factor).
-
-
OCT:
-
Confirms optic disc swelling; later shows RNFL thinning.
-
-
Fluorescein angiography:
-
Delayed or absent filling of the optic disc without choroidal hypoperfusion.
-
Differential Diagnosis
-
Arteritic AION (giant cell arteritis)
-
Optic neuritis
-
Compressive optic neuropathy
-
Leber hereditary optic neuropathy
-
Central retinal artery occlusion
-
Acute angle-closure glaucoma
Diagnosis
NAION is diagnosed clinically based on the combination of:
-
Sudden, painless monocular vision loss.
-
Optic disc swelling in the acute phase.
-
Corresponding visual field defect.
-
Presence of vascular risk factors.
-
Absence of systemic symptoms of giant cell arteritis and normal ESR/CRP.
No single test confirms NAION, but investigations such as OCT, visual fields, fluorescein angiography, and blood work (ESR/CRP) are used to exclude other causes.
Management
There is no proven treatment that reverses vision loss in NAION. Management focuses on preventing further episodes and optimizing systemic health:
-
Control of vascular risk factors:
-
Strict glycemic control in diabetics.
-
Blood pressure optimization (avoid excessive nocturnal lowering).
-
Lipid control.
-
-
Sleep apnea evaluation and treatment.
-
Aspirin: Sometimes prescribed for vascular protection, though evidence for preventing NAION in the fellow eye is inconclusive.
-
Patient education:
-
Risk of recurrence in the fellow eye is 15–25% over 5 years.
-
Need for regular follow-up.
-
Prognosis
Visual recovery in NAION is generally limited. About 40% of patients experience some improvement, but most retain some degree of field loss.
The fellow eye may be affected over time, particularly if risk factors are uncontrolled. NAION is non-progressive in the affected eye after the acute phase, but optic atrophy develops as the swelling resolves.

Prevention
-
Control of systemic hypertension, diabetes, and hyperlipidemia.
-
Avoidance of excessive nocturnal hypotension (review timing of antihypertensives).
-
Treatment of sleep apnea.
-
Smoking cessation.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Hayreh SS, Zimmerman MB. Non-arteritic anterior ischemic optic neuropathy: natural history of visual outcome. Ophthalmology. 2008;115(2):298–305.
-
Arnold AC. Pathogenesis of nonarteritic anterior ischemic optic neuropathy. J Neuroophthalmol. 2003;23(2):157–163.
-
Biousse V, Newman NJ. Ischemic optic neuropathies. N Engl J Med. 2015;372(25):2428–2436.

{kind=link}