

Case Study
A 29-year-old female presented with acute onset of blurred vision and periocular pain in her right eye, worsened by eye movement.


She reported that symptoms developed over 48 hours, with a rapid decline in visual acuity. She had no history of multiple sclerosis or autoimmune disease.
Examination Results
-
Visual Acuity: 20/200 (right eye), 20/20 (left eye)
-
Pupils: Right relative afferent pupillary defect (RAPD)
-
Color Vision: Impaired in the right eye
-
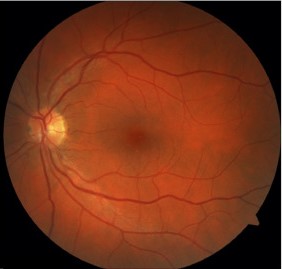
Fundus: Mild optic disc swelling in the right eye
-
MRI Orbit: T2 hyperintensity and contrast enhancement of the right optic nerve
-
Serum MOG-IgG: Positive by cell-based assay
A diagnosis of Myelin Oligodendrocyte Glycoprotein MOG-IgG Associated Optic Neuritis was established.
Disease Entity
Myelin Oligodendrocyte Glycoprotein (MOG)-IgG Associated Optic Neuritis is an inflammatory demyelinating condition of the optic nerve linked to antibodies against the MOG protein, located on the surface of myelin sheaths in the CNS.
Unlike optic neuritis in multiple sclerosis or neuromyelitis optica spectrum disorder (NMOSD), MOG-IgG-associated optic neuritis presents unique clinical and radiologic features, necessitating specific diagnosis and tailored treatment.
Pathophysiology
MOG is a CNS-specific glycoprotein expressed on the surface of oligodendrocytes and outermost myelin sheaths.
In MOG-IgG disease, circulating antibodies target MOG, leading to immune-mediated demyelination and inflammation.
Unlike multiple sclerosis, which involves T-cell-mediated mechanisms and CNS plaques, MOG-IgG optic neuritis is more often antibody-mediated and monophasic or relapsing in pattern.
The inflammatory response affects the optic nerve, resulting in visual loss and optic disc edema.
Epidemiology
MOG-IgG-associated optic neuritis can occur in both children and adults. It is slightly more common in females and can present as a monophasic illness or part of a relapsing disease.
Unlike MS-associated optic neuritis, MOG-related ON often involves bilateral presentation, optic disc edema, and poorer visual acuity at onset.
However, visual recovery is often better with appropriate therapy. The prevalence of MOG-IgG positivity in ON patients is estimated to be 5–25% depending on the population and diagnostic methods.
Clinical Features
-
Rapid onset of visual loss, often severe
-
Periocular pain, particularly with eye movement
-
Optic disc swelling, frequently bilateral
-
Color vision deficiency and central visual field defects
-
Positive MOG-IgG serology
-
May be recurrent or relapsing
-
In children, it may be associated with ADEM-like presentations
Examination Findings
-
Decreased visual acuity, often ≤20/200 at nadir
-
RAPD in unilateral cases
-
Optic disc edema on fundoscopy (frequent)
-
Visual field defects (central or altitudinal scotomas)
-
MRI: Optic nerve swelling and enhancement, often long-segment and anterior
-
CSF: May show mild pleocytosis, rarely oligoclonal bands
-
Serum: MOG-IgG positive by live cell-based assay
Differential Diagnosis
-
Multiple Sclerosis (MS)-related optic neuritis
-
Neuromyelitis Optica Spectrum Disorder (AQP4-IgG positive)
-
Infectious optic neuritis (e.g., syphilis, Lyme disease)
-
Sarcoidosis-associated optic neuropathy
-
Ischemic optic neuropathy (AION/NAION)
Diagnosis
-
Clinical presentation: acute, painful visual loss
-
MRI brain and orbit with contrast
-
Serum MOG-IgG testing by live cell-based assay
-
Lumbar puncture may help rule out other demyelinating or infectious causes
-
Visual evoked potentials (VEP) and OCT may be supportive
Management
-
Acute Phase:
-
High-dose IV methylprednisolone (1g/day for 3–5 days)
-
Consider plasma exchange (PLEX) if poor response
-
-
Long-term management (for relapsing disease):
-
Oral immunosuppressants (e.g., azathioprine, mycophenolate mofetil)
-
Rituximab or IVIG in some cases
-
-
Avoid MS-specific drugs like interferon-beta, which may worsen MOG disease
Prognosis
-
Visual recovery is generally good if treated early
-
Relapses are common; up to 50% of patients may experience recurrence
-
Long-term monitoring and serologic testing may be needed
-
Recurrence can be minimized with appropriate maintenance immunotherapy

Prevention
-
No known way to prevent the onset of MOG-IgG disease
-
Early recognition and prompt treatment of relapses
-
Maintenance immunosuppression in relapsing cases
-
Regular ophthalmologic follow-up with OCT and visual field testing
Conclusion
MOG-IgG-associated optic neuritis is a distinct clinical entity with unique immunopathological features.
Differentiating it from MS and NMOSD is crucial, as management strategies and prognosis differ significantly.
Prompt diagnosis using serological and radiologic tools, combined with early initiation of therapy, offers the best chance for visual recovery and long-term disease control.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Jarius S, et al. MOG encephalomyelitis: international recommendations on diagnosis and antibody testing. J Neuroinflammation.
-
Chen JJ, et al. Distinguishing MOG-IgG from AQP4-IgG optic neuritis. Neurology.
-
Hacohen Y, et al. MOG antibody-associated demyelinating disease in children. Neurology.
-
Narayan R, et al. MOG antibody disease: A review of clinical spectrum. Ann Indian Acad Neurol.
-
Reindl M, et al. Myelin oligodendrocyte glycoprotein antibodies: How clinical presentations differ. Curr Opin Neurol.

{kind=link}