
Optic disc swelling is a critical finding in ophthalmology that necessitates careful evaluation to determine its etiology.

While papilledema is often the first concern when optic disc swelling is observed, not all cases of optic disc swelling are due to papilledema.

Differentiating between papilledema and other causes of optic disc edema is essential, as misdiagnosis can lead to unnecessary interventions or a failure to detect potentially serious underlying conditions.
This article explores the various causes of optic disc swelling, the distinguishing features of papilledema, and approaches to accurate diagnosis and management.
Understanding Papilledema
Papilledema refers specifically to optic disc swelling due to increased intracranial pressure (ICP). This condition is typically bilateral, though asymmetric cases can occur.
The increased pressure in the subarachnoid space surrounding the optic nerve leads to axoplasmic flow stasis, causing swelling of the optic nerve head.
Common Causes of Papilledema:
- Idiopathic intracranial hypertension (IIH)
- Brain tumors (primary or metastatic)
- Hydrocephalus
- Meningitis or encephalitis
- Cerebral venous sinus thrombosis
- Severe hypertension (hypertensive encephalopathy)
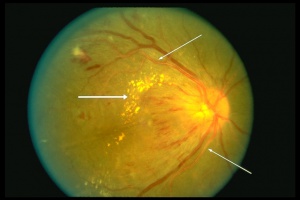
Clinical Features of Papilledema:
- Bilateral optic disc swelling
- Blurred disc margins with elevation
- Venous congestion and hemorrhages
- Cotton-wool spots and exudates (in advanced stages)
- Patency of the central cup in early cases
- Progressive vision loss, particularly peripheral vision
- Headache, nausea, vomiting, and transient visual obscurations
Other Causes of Optic Disc Swelling
While papilledema is a serious concern, various other conditions can also cause optic disc swelling. These conditions can be broadly classified into:
1. Optic Neuritis
Optic neuritis is inflammation of the optic nerve, commonly associated with demyelinating diseases such as multiple sclerosis (MS).

Unlike papilledema, optic neuritis is typically unilateral and presents with acute vision loss and pain in eye movement.
Key Differentiating Features:
- Unilateral in most cases
- Pain with eye movement
- Central or paracentral scotoma
- Relative afferent pupillary defect (RAPD)
- Normal or mildly elevated ICP
2. Anterior Ischemic Optic Neuropathy (AION)
AION results from compromised blood flow to the optic nerve head and can be classified into arteritic (associated with giant cell arteritis) and non-arteritic forms.
Key Differentiating Features:
- Sudden, painless vision loss
- Altitudinal visual field defects
- Optic disc pallor in chronic stages
- Systemic symptoms in arteritic AION (e.g., headache, jaw claudication, scalp tenderness)
3. Diabetic Papillopathy
This is a form of optic disc swelling seen in diabetic patients without significant visual loss.
Key Differentiating Features:
- Mild, non-progressive disc swelling
- Minimal or no visual symptoms
- Absence of hemorrhages or exudates
4. Hypertensive Optic Neuropathy
Chronic or malignant hypertension can cause optic disc swelling due to vascular changes in the optic nerve.
Key Differentiating Features:
- Bilateral disc swelling with flame-shaped hemorrhages
- Cotton-wool spots
- Presence of systemic hypertension
- Gradual visual deterioration
5. Compressive Optic Neuropathy
Tumors, aneurysms, or other compressive lesions along the visual pathway can cause optic disc swelling, usually with gradual progressive vision loss.
Key Differentiating Features:
- Progressive vision loss over weeks to months
- Proptosis (if orbital involvement)
- Visual field defects corresponding to lesion location
- Absence of increased ICP symptoms
6. Toxic or Nutritional Optic Neuropathy
Toxins (e.g., methanol, ethambutol) and nutritional deficiencies (e.g., B12 deficiency) can lead to optic neuropathy with swelling.
Key Differentiating Features:
- Bilateral, symmetric optic neuropathy
- Central or cecocentral scotomas
- Gradual, painless vision loss
- History of exposure to toxins or nutritional deficiencies
Diagnosis of Optic Disc Swelling
Given the diverse causes of optic disc swelling, a systematic approach to diagnosis is crucial.
1. Clinical History
- Onset and duration of symptoms
- Presence of headache, nausea, or vomiting (suggestive of increased ICP)
- History of systemic conditions (hypertension, diabetes, autoimmune diseases)
- Medication and toxin exposure history
2. Ophthalmic Examination
- Visual acuity and color vision testing
- Fundoscopy: Assess for disc elevation, hemorrhages, exudates
- Pupillary reactions (RAPD in unilateral optic neuropathies)
- Visual field testing (central scotomas in optic neuritis, altitudinal defects in AION)
3. Neuroimaging
- MRI/MRV brain and orbits: To rule out space-occupying lesions, sinus thrombosis, and demyelination
- CT scan: To assess for hydrocephalus or hemorrhage
4. Lumbar Puncture
- Required if IIH is suspected (opening pressure measurement and CSF analysis)
- Contraindicated in cases of mass lesions causing increased ICP
5. Laboratory Tests
- ESR, CRP for suspected giant cell arteritis
- Blood glucose and HbA1c for diabetic papillopathy
- B12, folate levels for nutritional optic neuropathies
- Toxin screening in suspected toxic optic neuropathy
Management Approaches
1. Papilledema
- Treat underlying cause (e.g., IIH with acetazolamide, weight loss; hydrocephalus with shunting)
- Close monitoring of visual fields
- Neurosurgical referral if required
2. Optic Neuritis
- High-dose corticosteroids for MS-associated optic neuritis
- Neurology referral for long-term management
3. AION
- Immediate steroids for arteritic AION (to prevent vision loss in the other eye)
- Control of vascular risk factors in non-arteritic AION
4. Hypertensive Optic Neuropathy
- Aggressive blood pressure control
5. Compressive Optic Neuropathy
- Surgery or radiotherapy for tumors
- Ophthalmic and neurology/neurosurgery consultation
6. Toxic and Nutritional Optic Neuropathy
- Discontinuation of toxic agents
- Nutritional supplementation and lifestyle changes
Conclusion
While optic disc swelling is a significant finding, it is not synonymous with papilledema. A thorough assessment is crucial to differentiate between papilledema and other optic neuropathies, as management strategies vary widely.
Misdiagnosis can lead to either unnecessary investigations or delayed treatment of potentially life-threatening conditions.
By employing a systematic approach, ophthalmologists can ensure accurate diagnosis and optimal patient care.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Friedman DI, Liu GT, Digre KB. “Papilledema and Pseudopapilledema: Recognition and Management.” J Neuroophthalmol. 2014;34(3):288-304.
- Biousse V, Newman NJ. “Neuro-Ophthalmology of Optic Neuritis.” Handb Clin Neurol. 2014;121:491-510.
- Hayreh SS. “Ischemic Optic Neuropathies.” Indian J Ophthalmol. 2000;48(3):171-194.
- Wall M, White W. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Diagnosis, Management, and Future Directions.” Neurol Clin. 2017;35(1):59-76.
- Wong TY, Mitchell P. “Hypertensive Retinopathy.” N Engl J Med. 2004;351(22):2310-2317.

{kind=link}