

Case Study
A 45-year-old female presented with progressive difficulty in reading and mild central vision distortion over the past five years.

Her medical and systemic history was unremarkable, but she reported a family history of macular degeneration. Best-corrected visual acuity (BCVA) was 20/30 in both eyes.
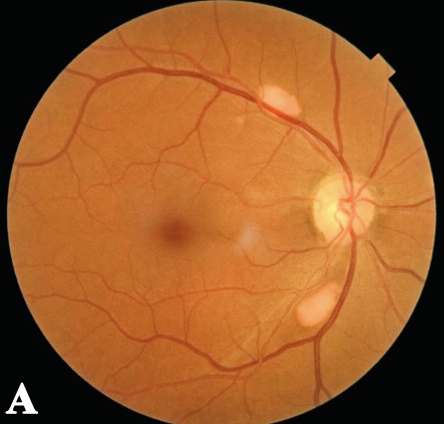
Fundus examination revealed multiple, yellowish, vitelliform lesions at the macula and posterior pole. Optical coherence tomography (OCT) showed hyperreflective deposits at the subretinal space, suggestive of Multifocal Vitelliform Dystrophy (MFVD).
Genetic testing confirmed a mutation in the BEST1 gene. The patient was advised on regular follow-ups, genetic counseling, and low-vision rehabilitation strategies.
Disease Entity
Multifocal Vitelliform Dystrophy (MFVD), also known as Adult-Onset Foveomacular Vitelliform Dystrophy, is a progressive retinal dystrophy characterized by bilateral, multiple, yellowish subretinal deposits resembling egg yolks.
It is part of the bestrophinopathies, affecting the retinal pigment epithelium (RPE) and photoreceptors, leading to gradual vision impairment.
MFVD shares similarities with Best disease but presents in adulthood and exhibits multiple vitelliform lesions.
Pathophysiology
MFVD results from mutations in the BEST1 or PRPH2 genes, leading to the dysfunction of bestrophin-1, a chloride channel essential for RPE health.
The disease progresses through several stages:
-
Early Stage:
- Accumulation of lipofuscin-like deposits in the subretinal space.
- Mild visual symptoms or asymptomatic.
-
Vitelliform Stage:
- Yellow lesions form in the macula, resembling Best disease but with multiple foci.
- Vision loss is mild to moderate.
-
Pseudohypopyon Stage:
- Gravity-dependent layering of vitelliform material.
- Lesions become more irregular.
-
Vitelliruptive Stage:
- Disruption of vitelliform material leads to mottled hyper/hypopigmentation.
- Patients experience a progressive visual decline.
-
Atrophic Stage:
- Photoreceptor loss and RPE atrophy lead to permanent central vision loss.

Epidemiology
- Onset: Typically in the 4th to 6th decade of life.
- Prevalence: Rare, but increasingly recognized with improved imaging techniques.
- Genetics: Autosomal dominant inheritance, primarily linked to BEST1 and PRPH2 mutations.
Clinical Features
Symptoms
- Mild to moderate vision loss (gradual progression).
- Metamorphopsia (distorted vision).
- Central or paracentral scotomas.
- Mild photophobia in some cases.
Fundoscopic Findings
- Bilateral yellow vitelliform lesions in the macula and posterior pole.
- Lesions can vary in size and shape, sometimes mimicking pattern dystrophies.
- RPE alterations with pigment clumping in later stages.
Imaging Findings
- Optical Coherence Tomography (OCT):
- Hyperreflective vitelliform deposits at the subretinal space.
- Progressive RPE thinning and photoreceptor loss in later stages.
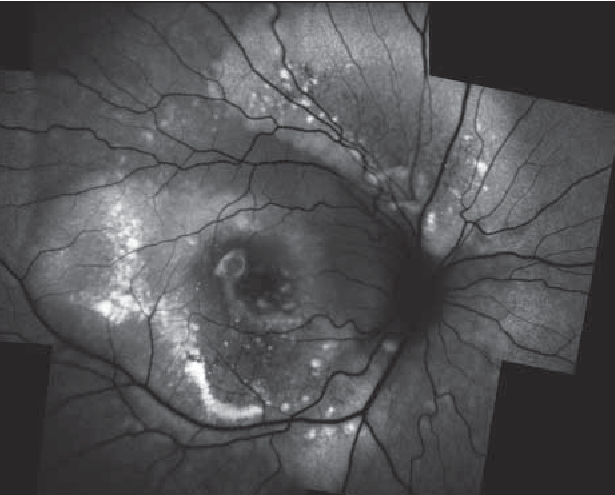
- Fundus Autofluorescence (FAF):
- Hyperautofluorescence in early lesions, with mottled autofluorescence in later stages.
- Fluorescein Angiography (FA):
- Minimal leakage (helps differentiate from inflammatory or exudative conditions).
Differential Diagnosis
- Best Disease: Typically presents in childhood with a single central lesion and different genetic inheritance.
- Age-Related Macular Degeneration (AMD): MFVD lacks drusen and choroidal neovascularization (CNV).
- Pattern Dystrophies: Some overlap in fundus appearance, but genetic and imaging studies can differentiate.
- Central Serous Chorioretinopathy (CSCR): Presence of subretinal fluid without characteristic vitelliform deposits.
- Stargardt Disease: Presence of pisciform flecks and earlier age of onset.
Diagnosis
- Clinical history and family history are crucial.
- Multimodal imaging (OCT, FAF, FA) is essential for diagnosis.
- Genetic testing (BEST1, PRPH2 mutations) for confirmation in uncertain cases.
Management
Observation and Monitoring
- Regular follow-up with OCT and FAF to track disease progression.
- Amsler grid monitoring at home for early detection of visual changes.
Supportive Care
- Low-Vision Aids: Magnifiers, contrast-enhancing filters.
- Blue-Light Blocking Lenses: May reduce phototoxicity effects.
- Nutritional Supplements: Lutein, zeaxanthin, and omega-3 fatty acids may provide some retinal protection.
Interventional Options
- Anti-VEGF Therapy: If CNV develops as a complication.
- Gene Therapy: Currently under investigation.
Prognosis
- Variable disease course: Some patients maintain relatively stable vision, while others progress to severe vision loss.
- Slower progression compared to other dystrophies, but irreversible atrophic changes can occur in later stages.
Conclusion
Multifocal Vitelliform Dystrophy is a progressive retinal dystrophy caused by genetic mutations affecting the retinal pigment epithelium and photoreceptors.
It presents with bilateral vitelliform deposits, gradual visual decline, and distinct OCT features. Diagnosis relies on multimodal imaging and genetic analysis, with management focusing on monitoring, low-vision rehabilitation, and potential future gene therapies.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Boon CJ, Klevering BJ, Keunen JE, et al. “Retinal dystrophies associated with mutations in the BEST1 gene.” Prog Retin Eye Res. 2009;28(3):187-205.
- Meunier I, Manes G, Bocquet B, et al. “Frequency and clinical patterns of bestrophinopathy associated with PRPH2 mutations.” Retina. 2015;35(7):1402-1411.
- Battaglia Parodi M, Romano F, Bandello F. “Multimodal imaging in vitelliform dystrophies.” Ophthalmologica. 2019;241(4):233-245.
- Sodi A, Passerini I, Murro V, et al. “BEST1 and PRPH2 mutations in adult-onset vitelliform macular dystrophy: A long-term retrospective study.” Retina. 2018;38(6):1200-1211.

{kind=link}