
Case Study
A 68-year-old woman presented with gradual deterioration of her night vision and difficulty seeing in dimly lit environments.


She also reported mild blurriness in her central vision. Her medical history included controlled hypertension and mild hypercholesterolemia, but no significant family history of eye disease.
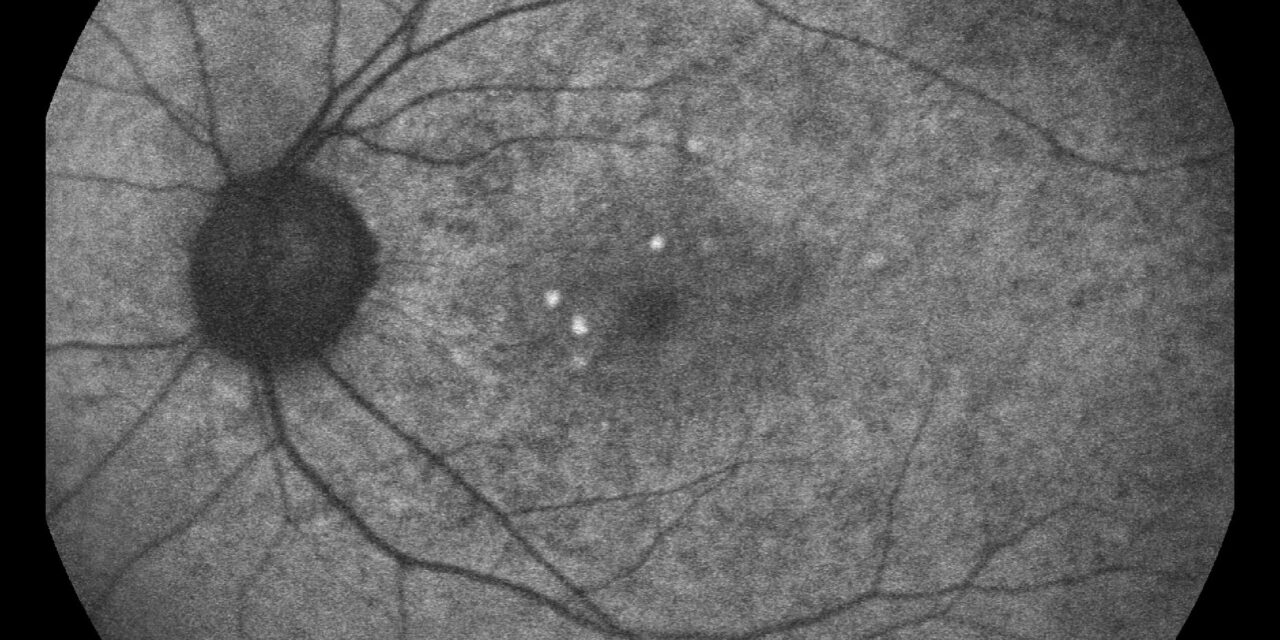
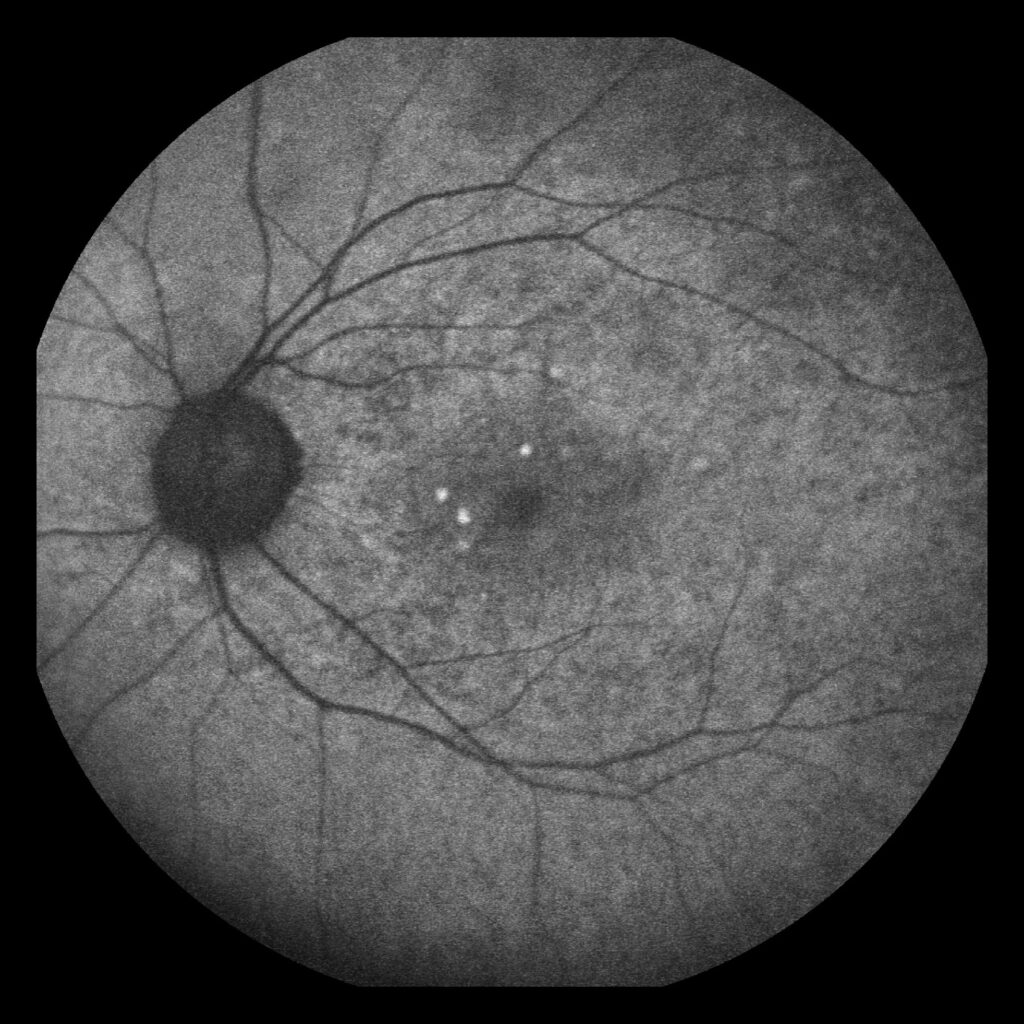
Fundus examination revealed numerous yellowish, interlacing deposits in the perifoveal region of both eyes, resembling a reticular pattern.
Optical coherence tomography (OCT) imaging demonstrated hyperreflective deposits above the retinal pigment epithelium (RPE), consistent with reticular pseudodrusen (RPD).
Fluorescein angiography and indocyanine green angiography confirmed the findings, and the patient was diagnosed with Reticular pseudodrusen associated with early age-related macular degeneration (AMD).
Disease Entity
Reticular pseudodrusen (RPD), also known as subretinal drusenoid deposits (SDD), are distinct deposits located above the RPE in the subretinal space.
Unlike conventional drusen, which are a hallmark of AMD, RPD is associated with distinct pathophysiological mechanisms and is considered a risk factor for advanced AMD, including geographic atrophy and neovascular AMD.
Pathophysiology
The precise mechanism behind RPD formation remains unclear, but it is thought to involve:
- RPE Dysfunction: Degeneration of RPE cells impairs the clearance of metabolic waste, leading to subretinal accumulation.
- Choroidal Hypoperfusion: Reduced blood flow in the choroidal vasculature may contribute to the development of RPD.
- Retinal Aging: Oxidative stress and chronic inflammation play significant roles in aging-related retinal changes, predisposing to RPD.
RPD deposits primarily consist of lipid-rich material, distinct from the extracellular matrix components of conventional drusen.
Epidemiology
- Prevalence: RPD is commonly seen in older adults, with prevalence increasing significantly after the age of 60.
- Association with AMD: Found in 20–30% of patients with AMD and strongly linked to advanced stages.
- Sex Distribution: More common in females, likely due to hormonal and vascular differences.
- Risk Factors: Includes advanced age, systemic hypertension, hyperlipidemia, and genetic predisposition (e.g., variants in the CFH and ARMS2 genes).
Clinical Features
RPD is characterized by its unique appearance and distinct anatomical location.
Symptoms:
- Early Stages: Often asymptomatic.
- Progressive Disease: Complaints of nyctalopia (night blindness), reduced contrast sensitivity, and difficulty adapting to low light conditions.
- Advanced Disease: Vision loss due to complications such as geographic atrophy or choroidal neovascularization.
Fundoscopic Appearance:
- Multiple small, yellowish deposits are arranged in an interlacing or reticular pattern, typically in the perifoveal or macular regions.
Diagnostic Evaluation
Imaging is critical for diagnosing RPD and differentiating it from other retinal conditions.
Fundus Examination:
- Yellow, reticular-patterned deposits are most prominent in the superior macula.
OCT:
- Hyperreflective material above the RPE in the subretinal space.
- Thinning of the RPE and outer retina in advanced stages.
FAF (Fundus Autofluorescence):
- Hypoautofluorescent spots are surrounded by a hyperautofluorescent halo, corresponding to RPD.
Indocyanine Green Angiography (ICGA):
- Hypofluorescent areas corresponding to choroidal hypoperfusion.
Multimodal Imaging:
Combining these techniques allows precise localization and monitoring of RPD.
Differential Diagnosis
Conditions that may mimic RPD include:
- Conventional Drusen: Located beneath the RPE, unlike the subretinal location of RPD.
- Pattern Dystrophy: Displays pigmentary changes rather than lipid-rich deposits.
- Central Serous Chorioretinopathy (CSC): Associated with serous detachments without reticular deposits.
- Stargardt Disease: Features flecks and atrophy rather than interlacing deposits.
Association with AMD
RPD is a significant biomarker for AMD progression, especially in developing advanced forms.
- Geographic Atrophy: RPD is frequently observed in the atrophic areas of AMD patients.
- Neovascular AMD: RPD is associated with an increased risk of choroidal neovascularization.
Management
There is no specific treatment for RPD itself; however, management focuses on monitoring progression and mitigating the risk of complications.
Risk Modification:
- Lifestyle Changes: Smoking cessation, dietary supplementation with antioxidants (AREDS2 formula), and blood pressure control.
- Monitoring: Regular ophthalmic evaluations, particularly for patients with a high risk of advanced AMD.
Advanced Disease:
- Anti-VEGF Therapy: For neovascular AMD.
- Low Vision Aids: In cases of vision impairment due to geographic atrophy.
Investigational Therapies:
- Photobiomodulation: Emerging as a potential intervention for AMD-related RPD.
- Choroidal Blood Flow Modulation: Research aims to improve choroidal perfusion to prevent RPD formation.

Prognosis
RPD presence indicates a heightened risk for advanced AMD, including significant central vision loss. Early detection, close monitoring, and lifestyle modifications can delay disease progression and preserve visual function.
Conclusion
Reticular pseudodrusen is a critical biomarker for AMD, reflecting subretinal changes that increase the risk of advanced complications.
Advances in imaging and research have improved our understanding of this condition, enabling earlier diagnosis and better monitoring.
Managing associated risk factors and regular follow-ups are essential for optimizing patient outcomes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Smith RT, Sohrab MA, Pumariega NM, et al. Reticular macular disease. Ophthalmology. 2011;118(7):1409-1415.
- Borrelli E, Abdelfattah NS, Uji A, et al. In vivo analysis of RPD using multimodal imaging. Retina. 2017;37(3):526-536.
- Ferrara D, Silver RE, Louzada RN, et al. Biomarkers of progression in AMD: The role of RPD. Progress in Retinal and Eye Research. 2020;76:100810.
- Zweifel SA, Imamura Y, Spaide TC, et al. Prevalence and significance of RPD in AMD. Investigative Ophthalmology & Visual Science. 2010;51(11):5608-5615.
- Curcio CA, Sloan KR, Millican CL, et al. Drusen and RPD: Two sides of the same coin? Archives of Ophthalmology. 2005;123(3):329-336.

{kind=link}