
Case Study
A 42-year-old woman presented with mild visual disturbances in her right eye, including blurry central vision and difficulty reading.

Her symptoms began gradually, with no significant pain or redness. She reported no medical issues but revealed that her father had experienced progressive vision loss in later years.
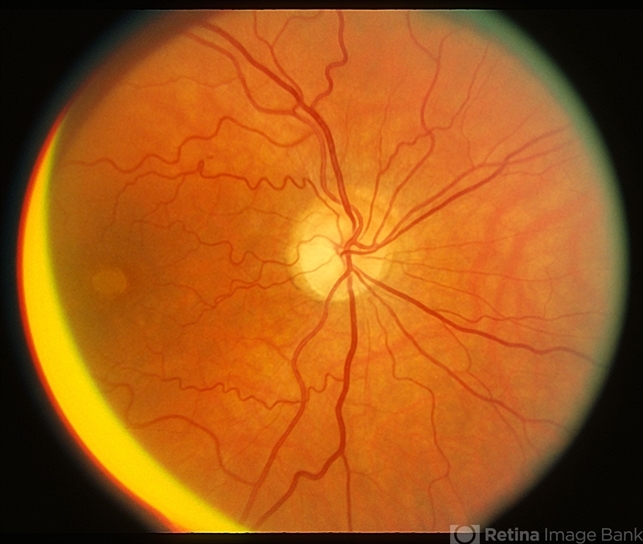
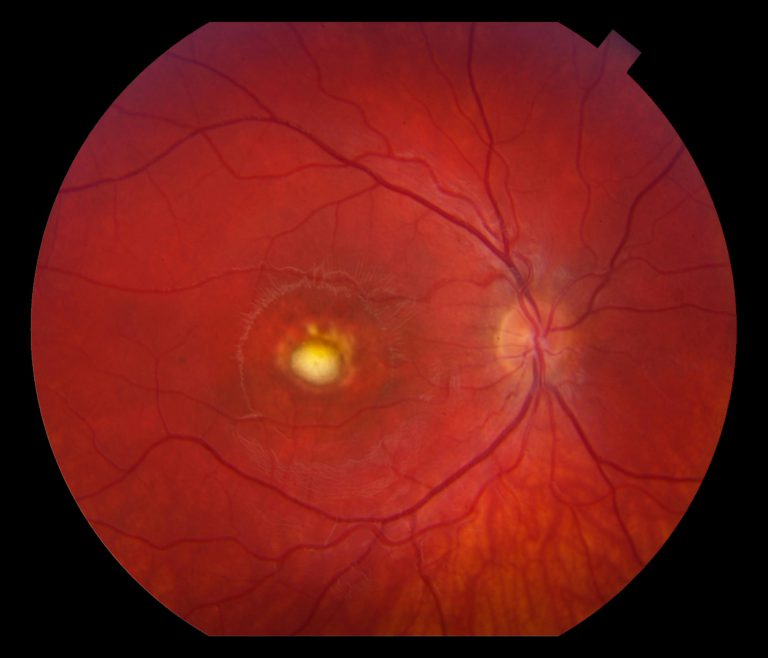
Fundus examination revealed a well-circumscribed, yellowish lesion resembling an egg yolk in the macula of her right eye. Her visual acuity was 20/30 in the affected eye and 20/20 in the left eye.
Optical coherence tomography (OCT) showed subretinal material accumulation at the level of the retinal pigment epithelium (RPE).
Electrooculography (EOG) demonstrated a low Arden ratio, supporting RPE dysfunction. Genetic testing confirmed a mutation in the BEST1 gene, leading to a diagnosis of vitelliform macular dystrophy (VMD).
Disease Entity
Vitelliform macular dystrophy (VMD), also known as Best disease or adult-onset vitelliform macular dystrophy, is a rare hereditary retinal disorder characterized by the accumulation of yellowish subretinal deposits in the macula.
These deposits, resembling an egg yolk, lead to progressive central vision loss, while peripheral vision typically remains unaffected. VMD is primarily an inherited condition, though sporadic cases have also been reported.
Pathophysiology
The hallmark of VMD is the dysfunction of the retinal pigment epithelium (RPE) caused by mutations in the BEST1 gene.
The encoded protein, bestrophin-1, is essential for maintaining ionic and fluid balance within the subretinal space.
Key pathological mechanisms include:
- Ion Channel Dysfunction: Mutated bestrophin-1 impairs calcium-dependent chloride ion transport, disrupting the homeostasis of the RPE.
- Lipofuscin Accumulation: The inability of RPE cells to clear photoreceptor outer segments results in the buildup of lipofuscin-like material.
- RPE Atrophy: Chronic stress on the RPE leads to cellular degeneration, contributing to photoreceptor loss and vision decline.
- Choroidal Neovascularization: In advanced stages, neovascular membranes may form, further compromising visual function.

Epidemiology
- Prevalence: VMD is rare, affecting approximately 1 in 10,000 individuals globally.
- Inheritance: Autosomal dominant, though incomplete penetrance and variable expressivity are common.
- Onset:
- Best Disease: Typically manifests in childhood or adolescence.
- Adult-Onset VMD: Emerges in the third or fourth decade of life.
- Sex Distribution: Equally affects males and females.
Clinical Features
The clinical spectrum of VMD varies widely, depending on the stage and subtype of the disease.
Early Stages:
- Asymptomatic or mild symptoms such as blurred central vision.
- Fundoscopic appearance of a vitelliform lesion in the macula resembling an egg yolk.
Progressive Stages:
- Lesion undergoes fragmentation, creating a “scrambled egg” appearance.
- Gradual decline in central vision due to RPE atrophy.
Late Stages:
- Advanced retinal degeneration with severe central vision loss.
- Possible complications like choroidal neovascularization or geographic atrophy.
Disease Stages
VMD typically progresses through five distinct stages, first described in Best’s original observations:
- Previtelliform Stage: Normal fundus with abnormal EOG findings.
- Vitelliform Stage: Classic “egg yolk” lesion forms in the macula.
- Pseudohypopyon Stage: Lesion demonstrates a layered appearance as deposits settle.
- Vitelliruptive Stage: Fragmentation of deposits into a “scrambled egg” appearance.
- Atrophic Stage: Loss of the lesion, with RPE atrophy and severe vision decline.
Diagnostic Evaluation
Accurate diagnosis of VMD requires clinical evaluation, advanced imaging, and genetic testing.
Imaging Techniques:
- Fundus Photography: Reveals the characteristic vitelliform lesion.
- OCT: Provides cross-sectional imaging of the retina, showing subretinal deposits, RPE thinning, and photoreceptor changes.
- FAF (Fundus Autofluorescence): Highlights areas of lipofuscin accumulation.
- Fluorescein Angiography (FA): Identifies potential neovascular complications.
Functional Testing:
- EOG: Reduced Arden ratio (<1.5), a hallmark of VMD.
- ERG (Electroretinography): Typically normal, differentiating VMD from other dystrophies.
Genetic Testing:
- Identifies mutations in the BEST1 gene or other associated genes, aiding in confirming the diagnosis.
Differential Diagnosis
Conditions with similar presentations include:
- Stargardt Disease: Presence of yellow flecks and central atrophy.
- Pattern Dystrophy: Macular deposits with a butterfly-shaped or reticular configuration.
- Central Serous Chorioretinopathy: Characterized by serous detachment without yellowish lesions.
- AMD (Age-Related Macular Degeneration): Presence of drusen and RPE atrophy in older adults.
Management
There is no definitive cure for VMD, but management strategies aim to monitor progression and treat complications.
Observation
- Regular follow-up with fundus imaging and functional tests to monitor lesion changes.
Pharmacologic Therapy
- Anti-VEGF Agents: Intravitreal injections for choroidal neovascularization (e.g., ranibizumab, aflibercept).
Vision Rehabilitation
- Low Vision Aids: Magnifiers, screen readers, and other adaptive devices to improve quality of life.
Experimental Therapies
- Gene Therapy: Promising experimental approach targeting BEST1 mutations.
- Stem Cell Therapy: Research is underway to replace damaged RPE cells.
Prognosis
The prognosis of VMD depends on the subtype, age of onset, and presence of complications.
- Childhood-Onset Best Disease: Slow progression, with many patients retaining useful vision into adulthood.
- Adult-Onset VMD: Variable course, with earlier central vision loss in some cases.
- Complications: Choroidal neovascularization is a major cause of severe vision decline if untreated.
Conclusion
Vitelliform macular dystrophy is a rare but well-characterized hereditary retinal disorder that primarily affects central vision.
Advances in imaging, genetic testing, and experimental therapies have improved the understanding and management of this condition.
Early detection and regular monitoring are essential to mitigate complications and preserve vision.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Best F. Ueber eine hereditaere Maculaaffektion: Beiträge zur Vererbungslehre. Zentralblatt für Praktische Augenheilkunde. 1905;29:238-241.
- Marmorstein AD, Cross HE, Peachey NS. Functional roles of bestrophins in ocular epithelia. Progress in Retinal and Eye Research. 2009;28(3):206-226.
- Querques G, Zerbib J, Georges A, et al. Insights into the pathogenesis of adult-onset foveomacular vitelliform dystrophy. Investigative Ophthalmology & Visual Science. 2011;52(7):4484-4495.
- Boon CJ, Klevering BJ, Leroy BP, et al. The spectrum of ocular phenotypes caused by mutations in the BEST1 gene. Progress in Retinal and Eye Research. 2009;28(3):187-205.
- Strauss RW, Ho A, Muñoz B, et al. Best Disease Natural History Study. Ophthalmology Retina. 2022;6(3):236-244.

{kind=link}