
Case Study
A 25-year-old man presented with complaints of night blindness since childhood, gradually worsening peripheral vision, and sensitivity to light.

He also reported occasional shimmering lights in his vision. His visual acuity was reduced to 20/50 bilaterally.
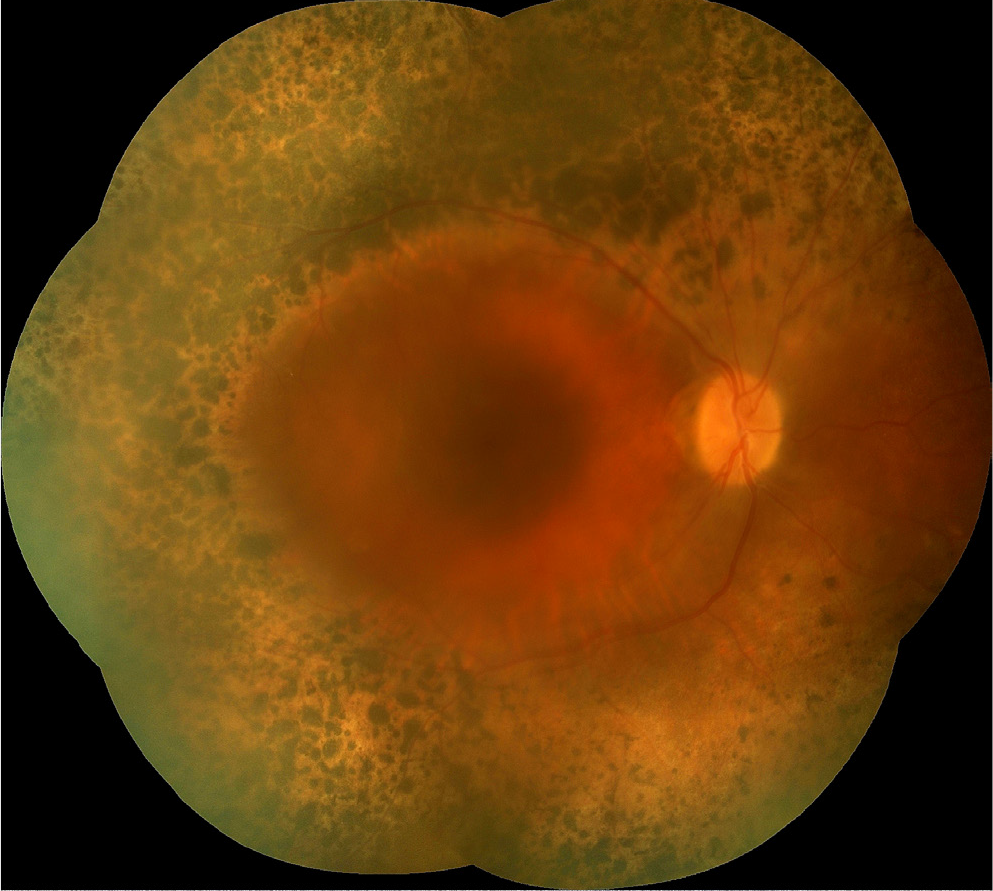
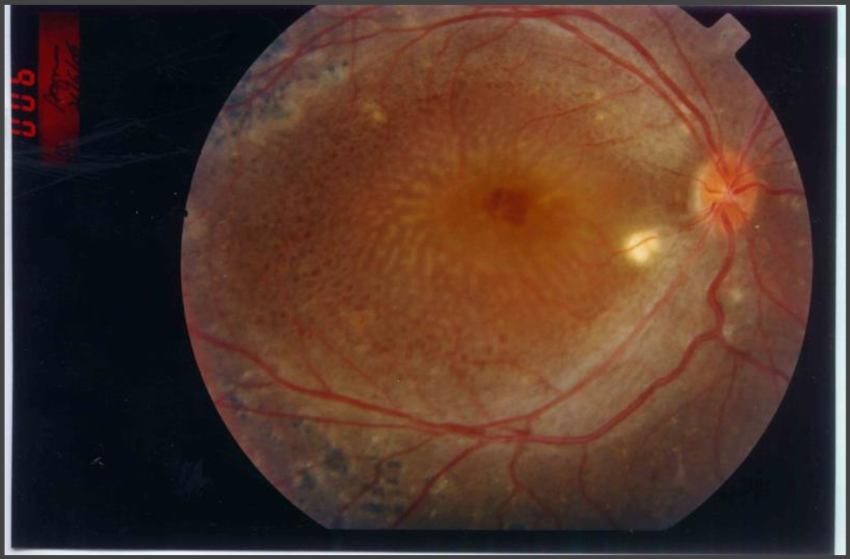
Fundus examination revealed widespread peripheral retinal degeneration with pigmentary changes and cystic macular edema.
Electroretinography (ERG) showed severely reduced rod and cone responses. Genetic testing confirmed a mutation in the NR2E3 gene, establishing a diagnosis of Goldmann-Favre syndrome.
Disease Entity
Goldmann-Favre syndrome is a rare inherited retinal dystrophy characterized by night blindness, progressive peripheral vision loss, cystoid macular edema, and retinal degeneration.
It is part of the enhanced S-cone syndrome (ESCS) spectrum due to mutations in the NR2E3 gene, which disrupts the normal balance of photoreceptors, leading to an overrepresentation of S-cones (short-wavelength cones).
Pathophysiology
Goldmann-Favre syndrome arises from mutations in the NR2E3 gene, which plays a critical role in retinal development and the differentiation of photoreceptor cells.
The genetic mutation disrupts the normal photoreceptor balance, leading to:
- Enhanced S-cone Function: An increased number of S-cones, which are abnormally sensitive to blue light.
- Rod and Cone Dysfunction: Reduced function of rod and long/middle-wavelength cones, resulting in night blindness and impaired peripheral vision.
- Progressive Retinal Degeneration: Degeneration of the peripheral retina with cystoid macular changes, contributing to central vision impairment over time.
Epidemiology
- Prevalence: Extremely rare, with only a few hundred cases reported globally.
- Inheritance: Autosomal recessive, requiring mutations in both copies of the NR2E3 gene for the disease to manifest.
- Demographics: Affects both genders equally, with symptoms typically presenting in childhood or early adulthood.

Clinical Features
- Night Blindness: Early-onset difficulty seeing in dim light or darkness.
- Peripheral Vision Loss: Progressive loss of peripheral visual fields due to retinal degeneration.
- Photophobia: Sensitivity to bright light, often exacerbated by the enhanced S-cone function.
- Visual Acuity Reduction: Gradual decline in central vision, often due to cystoid macular edema.
- Retinal Degeneration: Peripheral retinal atrophy, bone-spicule pigmentation, and vitreous opacities were observed on fundus examination.
- Electroretinography (ERG): Distinctive findings include severely reduced rod and cone responses with enhanced S-cone sensitivity.
Diagnosis
Diagnosis of Goldmann-Favre syndrome relies on a combination of clinical evaluation, imaging, and genetic testing:
- Fundus Examination: Reveals peripheral retinal atrophy, pigmentary changes, and cystoid macular edema.
- Electroretinography (ERG): Demonstrates enhanced S-cone function and diminished rod/cone activity.
- Optical Coherence Tomography (OCT): Identifies cystoid macular changes and thinning of the retinal layers.
- Genetic Testing: Confirms mutations in the NR2E3 gene.
Differential Diagnosis
Goldmann-Favre syndrome must be distinguished from other retinal dystrophies:
- Enhanced S-Cone Syndrome (ESCS): Shares many features with Goldmann-Favre syndrome but may present with milder macular involvement.
- Retinitis Pigmentosa (RP): Progressive rod and cone dystrophy without enhanced S-cone function.
- X-Linked Retinoschisis: Macular cystic changes with a splitting of the retinal layers, typically in males.
- Congenital Stationary Night Blindness (CSNB): Non-progressive night blindness without retinal degeneration.
Management
Goldmann-Favre syndrome is a progressive condition with no definitive cure. Management focuses on alleviating symptoms and preventing complications.
- Cystoid Macular Edema: Treated with carbonic anhydrase inhibitors (e.g., acetazolamide) or intravitreal corticosteroids in severe cases.
- Low Vision Aids: Devices such as magnifiers and enhanced lighting can help maximize remaining vision.
- Photoprotection: Tinted lenses to reduce photophobia and UV damage.
- Genetic Counseling: Educating patients and families about the inheritance pattern and implications.
Prognosis
The prognosis varies depending on the severity of macular involvement and rate of progression. Most patients experience a gradual decline in both central and peripheral vision, eventually leading to significant visual impairment.
Early diagnosis and intervention can help delay complications and optimize quality of life.
Conclusion
Goldmann-Favre syndrome is a rare autosomal recessive retinal dystrophy characterized by night blindness, peripheral vision loss, and macular edema.
It results from NR2E3 gene mutations, leading to enhanced S-cone function and progressive retinal degeneration.
While there is no cure, symptom management and supportive care can significantly improve patients’ quality of life.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Haider NB, Jacobson SG, Cideciyan AV, et al. Mutation of a nuclear receptor gene, NR2E3, causes enhanced S-cone syndrome, a disorder of retinal cell fate. Nature Genetics. 2000;24(2):127-131.
- Marmor MF, Cideciyan AV, Jacobson SG. Diagnostic challenges in enhanced S-cone syndrome and Goldmann-Favre syndrome. Investigative Ophthalmology & Visual Science. 2008;49(7):2820-2825.
- Audo I, Michaelides M, Robson AG, et al. Phenotypic variations of Goldmann-Favre syndrome in NR2E3 mutation carriers. British Journal of Ophthalmology. 2009;93(11):1524-1530.
- Fishman GA, Jampol LM, Goldberg MF. The Goldmann-Favre syndrome: A clinicopathologic study. Archives of Ophthalmology. 1976;94(1):34-43.
- Jacobson SG, Roman AJ, Aleman TS, et al. Short-wavelength cone sensitivity deficits in patients with Goldmann-Favre syndrome. Experimental Eye Research. 2004;79(5):495-505.

{kind=link}