
Case Study
A 45-year-old woman presented with persistent ocular discomfort and progressive vision deterioration in her right eye.

She reported intermittent episodes of eye pain exacerbated by head movements. Examination revealed a slightly proptotic right eye with a restricted upward gaze.
Imaging studies showed an irregularly shaped intraorbital mass with calcifications compressing the optic nerve.
The clinical and imaging findings led to a diagnosis of Crunch Syndrome, highlighting the critical need for timely surgical intervention to relieve optic nerve compression and prevent permanent visual impairment.
Disease entity
Crunch Syndrome, a rare but severe condition, occurs due to optic nerve compression caused by orbital masses. The syndrome gets its name from the “crunching” effect of calcified or rigid masses exerting mechanical pressure on orbital structures, leading to progressive visual dysfunction and discomfort.
Typically associated with various orbital pathologies, including tumors, cysts, or trauma-related masses, Crunch Syndrome requires prompt diagnosis and intervention to prevent permanent vision loss.
Pathophysiology
The primary mechanism of Crunch Syndrome is the mechanical compression of the optic nerve by an intraorbital mass.
- Direct Compression:
The mass physically impinges on the optic nerve, disrupting axonal transport and blood flow. Chronic compression can lead to ischemia and optic atrophy. - Secondary Effects:
- Inflammatory responses may exacerbate optic nerve damage.
- Restricted ocular motility is due to the mass effect on extraocular muscles.
- Calcified Lesions:
The rigid, non-compliant nature of calcified masses amplifies the compressive effects, leading to more severe symptoms.
Epidemiology
Crunch Syndrome is extremely rare, with cases reported in individuals of all age groups. It is often associated with underlying conditions, such as:
- Orbital tumors (e.g., meningiomas, hemangiomas).
- Post-traumatic orbital hematomas or bony fragments.
- Congenital anomalies like dermoid cysts or teratomas.
The prevalence is difficult to estimate due to the syndrome’s rarity and its frequent misclassification under broader orbital compression syndromes.
Clinical Features
The presentation of Crunch Syndrome varies depending on the size, location, and nature of the compressive lesion. Common features include:
- Visual Impairment:
Progressive loss of visual acuity and color vision is the hallmark. - Ocular Discomfort:
Patients may report dull pain, often worsened by eye movement or head position changes. - Proptosis:
Mild to moderate proptosis is frequently observed, depending on the mass size. - Restricted Ocular Motility:
Compression of extraocular muscles or mechanical limitation by the mass can cause diplopia or restricted gaze. - Optic Disc Changes:
- Early stages: Disc edema (papilledema).
- Late stages: Optic atrophy due to chronic compression.
Diagnosis
Timely diagnosis of Crunch Syndrome relies on clinical examination and imaging.
- Clinical Examination:
- Assess visual acuity, color vision, and pupillary response.
- Evaluate ocular motility and measure proptosis using exophthalmometry.
- Imaging:
- CT Scan: Identifies calcifications, bony deformities, or trauma-induced fragments.
- MRI: Provides detailed soft tissue visualization, delineating mass characteristics and optic nerve involvement.
- Differential Diagnosis:
Crunch Syndrome must be differentiated from other causes of optic neuropathy, including:- Thyroid eye disease.
- Orbital cellulitis or abscess.
- Idiopathic orbital inflammatory syndrome (orbital pseudotumor).
Management
Management of Crunch Syndrome focuses on relieving optic nerve compression and addressing the underlying pathology.
- Surgical Intervention:
- Orbital decompression is the primary treatment to alleviate pressure.
- Mass excision or biopsy may be necessary for definitive diagnosis and therapy.
- Medical Management:
- Systemic corticosteroids may be used to reduce inflammation, particularly in cases with an inflammatory component.
- Pain management with analgesics is often required.
- Postoperative Care:
- Regular monitoring of visual function and imaging follow-ups are critical.
- Rehabilitation for ocular motility issues may be needed.
- Treatment of Underlying Causes:
Addressing the specific etiology, such as radiation therapy for orbital tumors or antibiotics for infections, is vital to prevent recurrence.
Prognosis
The prognosis of Crunch Syndrome depends on the duration and severity of optic nerve compression at the time of diagnosis:
- Favorable Prognosis: Early diagnosis and timely intervention often result in significant visual recovery.
- Poor Prognosis: Chronic or prolonged compression may lead to irreversible optic atrophy and permanent vision loss.
Prevention
Preventing Crunch Syndrome involves early detection and management of orbital lesions:
- Regular ophthalmologic evaluations for individuals with known orbital pathologies.
- Timely imaging for unexplained proptosis or visual changes.
- Monitoring of post-traumatic orbital injuries to identify developing compressive masses.
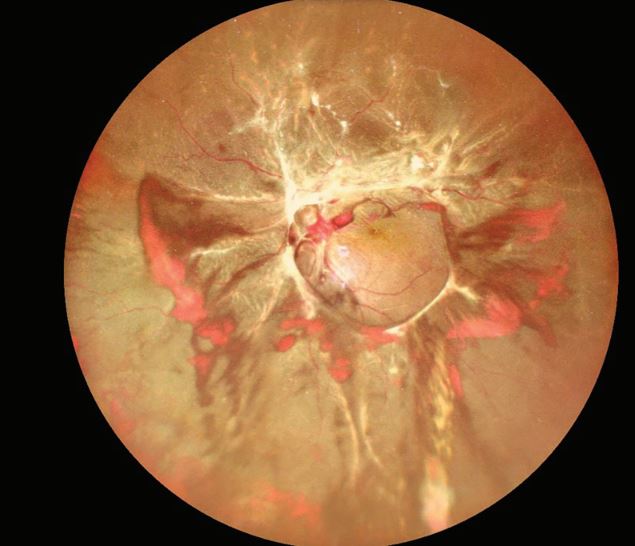
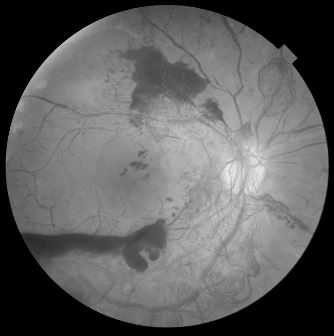
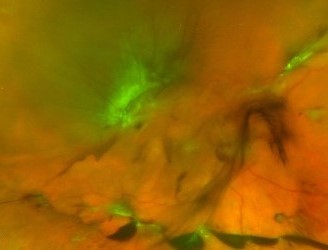
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Carter KD, Nerad JA. Orbital masses compressing the optic nerve: Clinical findings and management. Ophthalmic Plast Reconstr Surg. 2002;18(4):254-258.
- Shields CL, Shields JA. Orbital tumors: Diagnosis and management. Curr Opin Ophthalmol. 2010;21(5):367-373.
- Rootman J. Diseases of the Orbit: A Multidisciplinary Approach. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 2003.
- Yang M, Wei WB, Li H. Rare causes of orbital compression syndromes: Case series and review of literature. BMC Ophthalmol. 2020;20(1):97.

{kind=link}