
Case Study
A 43-year-old man with a history of HIV/AIDS and poor adherence to antiretroviral therapy presented with progressive vision loss and floaters in his left eye for three weeks.

He also reported intermittent headaches and neck stiffness. Fundoscopic examination revealed yellowish subretinal lesions with ill-defined borders in the posterior pole and peripapillary region, along with vitritis.
MRI of the brain showed basal meningeal enhancement, and cerebrospinal fluid (CSF) analysis revealed a positive India ink test and elevated cryptococcal antigen titers.
A diagnosis of cryptococcal choroiditis secondary to cryptococcal meningitis was made.
The patient was started on amphotericin B and flucytosine, followed by fluconazole maintenance therapy, with improvement in both systemic and ocular symptoms.
Disease entity
Cryptococcal choroiditis is a rare but potentially vision-threatening ocular manifestation of systemic cryptococcosis, primarily caused by Cryptococcus neoformans or Cryptococcus gattii.
It occurs most commonly in immunocompromised individuals, particularly those with advanced HIV/AIDS, organ transplantation, or other conditions leading to impaired cellular immunity.
The infection typically arises as a disseminated disease, with the choroid becoming involved via hematogenous spread.
Early recognition and treatment are essential to prevent irreversible vision loss and systemic complications.
Pathophysiology
Cryptococcal choroiditis results from hematogenous dissemination of Cryptococcus species, which are encapsulated yeast pathogens. Key mechanisms include:
- Hematogenous Spread:
- Fungal spores disseminate to the choroid via systemic circulation.
- Choroidal Localization:
- The high vascularity of the choroid makes it a common site for fungal seeding.
- Granulomatous Inflammation:
- Cellular immune response leads to granuloma formation and subretinal lesions.
- Neuroretinal Involvement:
- Progression can lead to optic nerve involvement, vitritis, and retinal detachment.
Epidemiology
- Prevalence:
- Cryptococcal infections are common in individuals with compromised immune systems but choroidal involvement is relatively rare.
- Risk Factors:
- HIV/AIDS with CD4 count <100 cells/µL.
- Prolonged corticosteroid use.
- Post-transplant immunosuppression.
- Sarcoidosis and other granulomatous diseases.
Clinical Features
Cryptococcal choroiditis presents with a variety of ocular and systemic symptoms:
- Ocular Symptoms:
- Blurred vision.
- Floaters.
- Photophobia.
- Pain in cases of concurrent scleritis or anterior uveitis.
- Systemic Symptoms:
- Headache, fever, and meningismus from cryptococcal meningitis.
- Skin lesions resembling molluscum contagiosum in disseminated disease.

Fundoscopic Findings
- Yellowish-white subretinal lesions with ill-defined borders.
- Peripapillary choroiditis.
- Vitritis and optic disc edema in advanced cases.
Examination Findings
- Slit-Lamp Examination:
- Rarely, anterior uveitis or keratic precipitates.
- Fundoscopy:
- Choroidal granulomas or diffuse choroidal thickening.
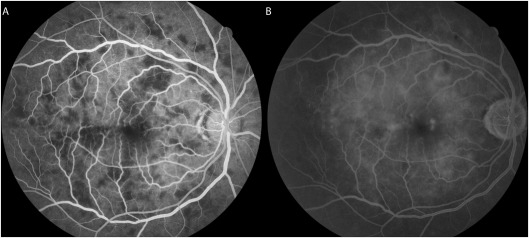
- Ocular Imaging:
- Optical coherence tomography (OCT): Shows hyperreflective subretinal deposits.
- Fluorescein angiography (FA): Highlights areas of choroidal hypoperfusion and leakage.
Differential Diagnosis
Cryptococcal choroiditis must be distinguished from other infectious and inflammatory conditions:
- Tuberculous choroiditis.
- Toxoplasmic chorioretinitis.
- Syphilitic choroiditis.
- Cytomegalovirus retinitis.
- Sarcoidosis-associated choroiditis.
Diagnosis
Diagnosis requires a combination of ocular and systemic investigations:
- Ocular Diagnostics:
- Fundoscopic examination and OCT for characteristic choroidal lesions.
- Systemic Investigations:
- CSF analysis with India ink staining and cryptococcal antigen testing.
- Serum cryptococcal antigen testing.
- Imaging:
- Brain MRI/CT to evaluate for cryptococcal meningitis or CNS involvement.
- Definitive Test:
- Culture of Cryptococcus from CSF, blood, or ocular fluids.
Management
Treatment of cryptococcal choroiditis involves systemic antifungal therapy alongside supportive ocular care:
- Antifungal Therapy:
- Induction: Amphotericin B plus flucytosine for at least 2 weeks.
- Consolidation: Fluconazole for 8–10 weeks.
- Maintenance: Long-term fluconazole for patients with ongoing immunosuppression.
- Ocular Interventions:
- Local corticosteroids for inflammatory sequelae (with caution to avoid exacerbating fungal growth).
- Pars plana vitrectomy in cases of persistent vitritis or retinal detachment.
- Supportive Care:
- Management of raised intracranial pressure with therapeutic lumbar punctures.
- Optimization of antiretroviral therapy in HIV/AIDS patients.

Prognosis
Early recognition and treatment significantly improve outcomes in cryptococcal choroiditis.
However, the prognosis depends on systemic immune status and timely control of CNS involvement.
- Untreated or delayed cases can result in permanent vision loss due to optic nerve damage or retinal detachment.
- Mortality remains high in disseminated cryptococcosis, emphasizing the need for a multidisciplinary approach.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Perfect, J. R., Dismukes, W. E., Dromer, F., et al. (2010). Clinical practice guidelines for the management of cryptococcal disease. Clinical Infectious Diseases, 50(3), 291–322.
- Tanabe, Y., Kato, T., & Yamamoto, H. (2001). Ocular manifestations of cryptococcosis. International Ophthalmology Clinics, 41(1), 167–176.
- Park, B. J., Wannemuehler, K. A., Marston, B. J., et al. (2009). Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS, 23(4), 525–530.
- Subramanian, S., & Mathai, D. (2005). Clinical manifestations and management of cryptococcal infection. Journal of Postgraduate Medicine, 51(5), S21–S26.
- Neumann, D., & Hagen, F. (2015). Ocular cryptococcosis: A case series and review of the literature. Medical Mycology Case Reports, 8, 11–16.


{kind=link}