
CASE REPORT
A 45-year-old male presented to an ophthalmology clinic with complaints of discomfort, redness, and a raised lesion on the sclera of his right eye, which had been bothering him for the past six weeks.


His medical history was unremarkable, with no prior ocular or systemic conditions, and he denied any history of trauma to the eye or exposure to irritants.
Initial examination revealed 20/20 visual acuity in both eyes, localized conjunctival injection, and a raised, pinkish-white nodule on the inferonasal quadrant of the right eye’s sclera, while the left eye showed no abnormalities.
Slit-lamp biomicroscopy confirmed the presence of a well-defined, non-mobile nodule on the sclera, with intact overlying conjunctiva and clear cornea and anterior chamber.
Intraocular pressure was within normal limits in both eyes, and fundus examination revealed no signs of pathology. Differential diagnoses included focal scleritis, scleral nodule of unknown origin, scleral tumor, and pterygium.
Further investigations, such as ultrasound biomicroscopy, laboratory tests, and a scleral nodule biopsy, were performed to establish the diagnosis, which confirmed the Focal Scleral Nodule (FSN).
Focal Scleral Nodule (FSN) DISEASE entity
A focal Scleral Nodule (FSN), previously referred to as solitary idiopathic choroiditis (SIC) and unifocal helioid choroiditis, is characterized by an inflammatory granulomatous reaction in the sclera and/or choroid in the absence of an underlying systemic inflammatory disease.
It is a rare condition found more commonly in white females between the ages of 20 and 50 and where approximately a third of patients are asymptomatic at the time of diagnosis. Current management recommendations of FSN suggest monitoring of inactive lesions and either close observation or treatment with systemic corticosteroids for active lesions.
Risk factors remain poorly understood likely due to the poor understanding of the pathogenesis. Several associations have been suggested including associations with systemic diseases such as tuberculosis, syphilis, sarcoidosis, cat scratch disease, and coxsackie virus.
However, this remains unclear and has been challenged in recent literature; no significant relation with these systemic conditions has been found.
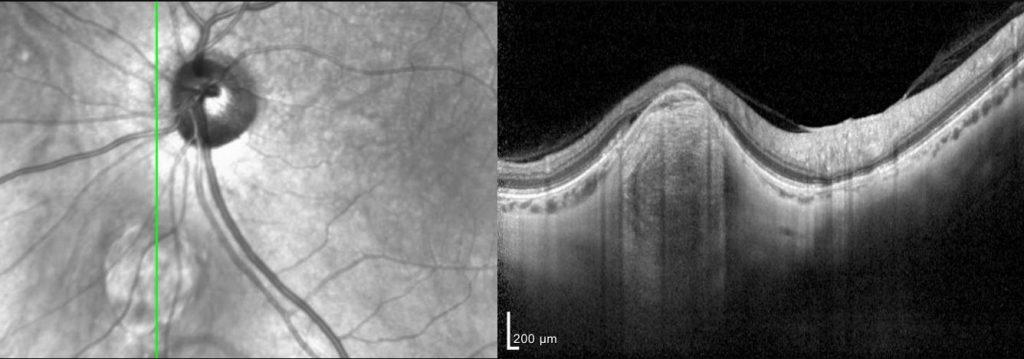
Optical coherence tomography (OCT) has led to a new understanding of Focal Scleral Nodule (FSN) including the anatomic origin in the sclera vs. the choroid as previously described. Most lesions have been revealed to have a dome shape, but nodular or volcanic shapes have also been noted.
The overlying choroid usually shows thinning or absence and is the likely cause of the orange halo seen on the fundoscopic exam. OCT angiography will show the lesions to be avascular and most will demonstrate hyperautofluorescence.
Focal Scleral Nodule (FSN) Differential diagnosis
Many lesions have a somewhat similar presentation to FSN. Some of these are benign while others may indicate a more urgent or dangerous disease.
A thorough exam and imaging are important to differentiate these lesions and many can be ruled out with OCT showing a scleral lesion vs. a lesion arising from the choroid.

The following lesions may present similarly:
- Choroidal metastasis
- Choroidal melanoma
- Choroidal lymphoma
- Retinoblastoma
- Astrocytic hamartoma
- Choroidal nevus
- Choroidal granuloma
- Choroidal scars
- White dot syndromes
- Sarcoidosis
- Ocular tuberculosis
- Ocular syphilis
- Fungal chorioretinitis
- Sclerchoroidal calcification
Focal Scleral Nodule (FSN) MANAGEMENT
When followed over time most lesions remain stable without changes. Nevertheless, there are reports of lesions that demonstrate growth or resolution with long-term follow-up.
Due to the benign nature and limited functional impact of an FSN, no treatment is indicated in most cases. In the event that a lesion does appear to be active with associated inflammation, systemic steroids have been suggested as a possible trial treatment.
However, there have been no studies evaluating the overall effectiveness of this treatment. Active lesions can respond favorably with or without steroid treatment.
Regardless, due to the potential danger of similar-looking lesions, it is imperative to correctly diagnose an FSN prior to informing a patient that they do not need follow-up care.
The potential erroneous diagnosis of an FSN in place of a choroidal metastasis or melanoma could be disastrous.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Hong PH, Jampol LM, Dodwell DG, Hrisomalos NF, Lyon AT. Unifocal helioid choroiditis. Arch Ophthalmol. 1997 Aug;115(8):1007-13.
- Shields JA, Shields CL, Demirci H, Hanovar S. Solitary Idiopathic Choroiditis: The Richard B. Weaver Lecture. Arch Ophthalmol. 2002;120(3):311–319.
- Fung AT, Kaliki S, Shields CL, Mashayekhi A, Shields JA. Solitary idiopathic choroiditis: findings on enhanced depth imaging optical coherence tomography in 10 cases. Ophthalmology. 2013;120:852–858
- Fung AT, Waldstein SM, Gal-Or O, Pellegrini M, Preziosa C, Shields JA, Welch RJ, Dolz-Marco R, Sarraf D, Nagiel A, Lalane R, Jung JJ, Ghazi NG, Ramtohul P, Arnold JJ, Sakurada Y, Choudhry N, Balaratnasingam C, Freund KB, Shields CL. Focal Scleral Nodule: A New Name for Solitary Idiopathic Choroiditis and Unifocal Helioid Choroiditis. Ophthalmology. 2020 Nov;127(11):1567-1577.
- Goyal S, Ware GT, Petrovic’ V. Coxsackie virus a possible missing link to unifocal helioid choroiditis? Clin Exp Ophthalmol. 2015 May-Jun;43(4):377-9.
- Kumar V, Khoo CT, Shields CL. Solitary idiopathic choroiditis in the setting of extensive animal exposure. Retin Cases Brief Rep. 2016 Fall;10(4):386-8.
- Feng Y, Conrady CD, Demirci H. The evolution of an active solitary idiopathic choroiditis (focal scleral nodule): a case report of the natural course and a review of the literature. BMC Ophthalmol. 2021;21(1):130. Published 2021 Mar 9. doi:10.1186/s12886-021-01888-5.

{kind=link}