
CASE REPORT
A 45-year-old male presented to an ophthalmology clinic with a chief complaint of visual disturbances and the presence of a central scotoma in his right eye.
He reported a gradual decline in visual acuity over the past two months. Notably, there was no history of ocular trauma or systemic illnesses, including diabetes or hypertension.
On ocular examination, the visual acuity in the right eye (OD) was measured at 20/200, while the left eye (OS) exhibited 20/20 vision.
Intraocular pressure measurements were within the normal range, with OD at 15 mmHg and OS at 16 mmHg.
In the posterior segment examination of the right eye (OD), a central scotoma was observed during Amsler grid testing.
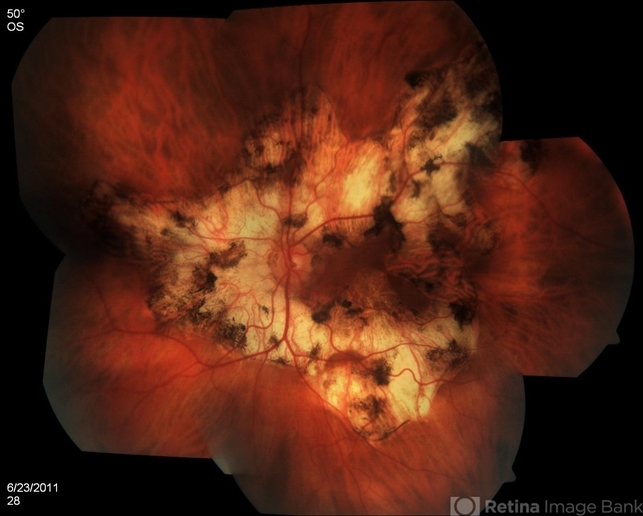
Additionally, mild vitritis was noted along with the presence of multiple yellow-white, deep choroidal lesions at the posterior pole, extending into the macular region.
This constellation of findings was consistent with active choroiditis and areas of serpiginous geographic atrophy. In contrast, the left eye (OS) demonstrated a normal retina and choroid.
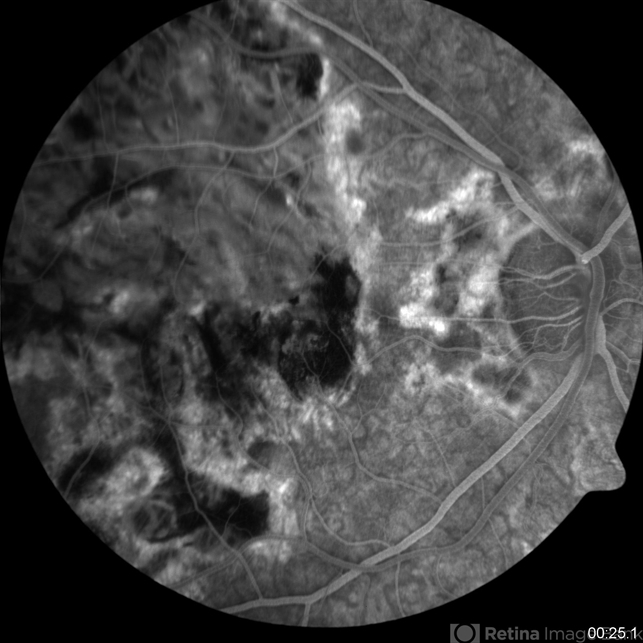
Diagnostic tests, including fluorescein angiography, indicated hyperfluorescence of the choroidal lesions in the late phase, with no evidence of active neovascularization. Optical coherence tomography further revealed subretinal fluid accumulation and outer retinal disruption in the macular area.
Based on the clinical presentation, ophthalmic examination, and diagnostic test results, the patient was diagnosed with Serpiginous Choroidopathy (SC).
Serpiginous Choroidopathy DISEASE entity
Serpiginous choroidopathy (SC) is a rare, bilateral, chronic, progressive, recurrent inflammatory disease of the retinal pigment epithelium (RPE), choriocapillaris, and choroid of unknown etiology.


SC is a rare clinical entity causing less than 5% of posterior uveitis cases. It has a higher prevalence in men and affects young to middle-aged adults. No systemic disease associations have been identified.
Patients present with painless unilateral vision loss, metamorphosis, or central scotoma.
Although of unknown etiology, its origin is probably immunogenic since it seems to respond to treatment with corticosteroids and other immunosuppressants. Moreover, affected patients also show an increased frequency of HLA-B7 and retinal S-antigen associations.
Other pathogenic mechanisms have been proposed and there may be an association with SC with infectious etiologies such as Mycobacterium tuberculosis and herpes viruses but this remains to be proven. Alternatively, SC and tuberculosis-related SC may be different disease entities with overlapping features.
Serpiginous Choroidopathy Diagnosis
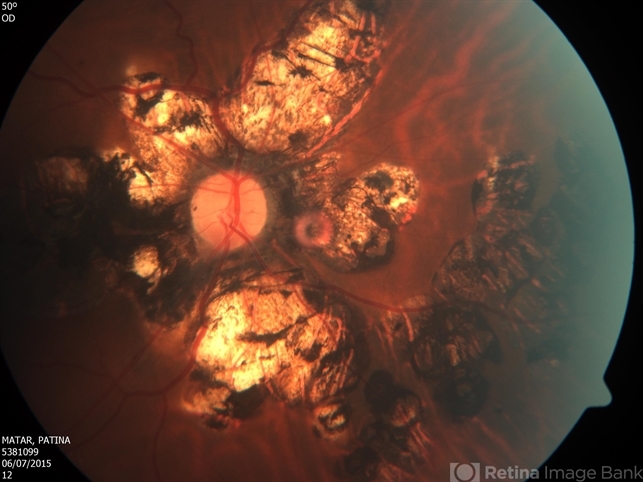
Serpiginous choroidopathy (SC) presents with gray-yellowish subretinal infiltrates that usually spread centrifugally from the peripapillary region in a serpiginous (snake-like) manner. Active lesions show a leading edge and resolve with subsequent RPE and choriocapillary atrophy.
Consecutive recurrences cause further atrophy leaving hypo- and hyper-pigmented lesions that spread irregularly over the posterior fundus. Although bilateral, the disease is often asymmetric with multiple lesions in different stages of resolution in both eyes.
Recurrences have variable intervals that range from months to years. Anterior chamber and vitritis are minimal.
The former begins as a macular lesion that spares the peripapillary region with a higher risk of choroidal neovascularization (CNV) and poor visual outcome.
Ampiginous chorioretinopathy is characterized by multifocal plaque-like lesions scattered over the posterior pole that have overlapping features of both acute posterior multifocal placoid pigment epitheliopathy (APMPPE) and SC.
Ampiginous chorioretinopathy is characterized by multiple recurrences and progressive enlargement of serpiginous lesions over time without the spontaneous resolution typical of APMPPE.
Serpiginous Choroidopathy MANAGEMENT
Treatment of Serpiginous choroidopathy (SC) aims to stop chorioretinal inflammation especially when the advancing lesions threaten the fovea.
Systemic or periocular corticosteroids are frequently used but recurrence prevention usually requires long-term anti-inflammatory treatment with a steroid-sparing agent, such as antimetabolites (methotrexate, mycophenolate mofetil, azathioprine), cyclosporine A, or anti-TNF agents, such as adalimumab or infliximab, once tuberculosis has been ruled out.
Long-term management can be challenging and up to 25% of the eyes have a final visual acuity of less than 20/200.
Complications
The most common complication of SC is choroidal neovascularization affecting up to 35% of patients. Other reported complications are subretinal fibrosis, cystoid macular edema, branch vein occlusion, serous retinal detachment, optic disc neovascularization, and anterior uveitis.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Bacin F, Larmande J, Boulmier A, Juliiar G. Serpiginous choroiditis and placoid epitheliopathy. Bull Soc Ophthalmol Fr. 1983; 83:1153-62.
- Abu el-Asrar AM. Serpiginous (geographical) choroiditis. Int Ophthalmol Clin. 1995; 35:87-91
- Ciulla TA, Gragoudas ES. Serpiginous choroiditis. Int Ophthalmol Clin. 1996; 36:135-43.
- Nazari Khanamiri H, Rao NA. Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis. Surv Ophthalmol. 2013 May-Jun;58(3):203-32.
- Gupta V, Gupta A, Arora S, Bambery P, Dogra MR, Agarwal A. Presumed tubercular serpiginous like choroiditis: clinical presentations and management. Ophthalmology. 2003 Sep;110(9):1744-9.

{kind=link}