
CASE REPORT
A 55 years old man who had been known to be diabetic for 16 years on a diet alone and hypertensive for 5 years on beta-blocker monotherapy. He had been suffering from intense headaches with photophobia for 48 h.

The situation was aggravated by the appearance of incoercible vomiting with a sudden drop in visual acuity in the right eye, without pain, leading to a consultation in the emergency room. The neurological examination showed a Glasgow score of 13/15, an apyretic meningeal syndrome, and a right hemiparesis with slight motor aphasia.
The emergency CT scan revealed a spontaneous meningeal hemorrhage due to a ruptured aneurysm of the right internal carotid artery at the level of its supra-clinoid segment. Complementary cerebral MRI confirms the subarachnoid hemorrhage and the appearance of the ruptured aneurysm.
The patient was managed neurosurgically the same day. The aneurysm was treated by embolization with success.
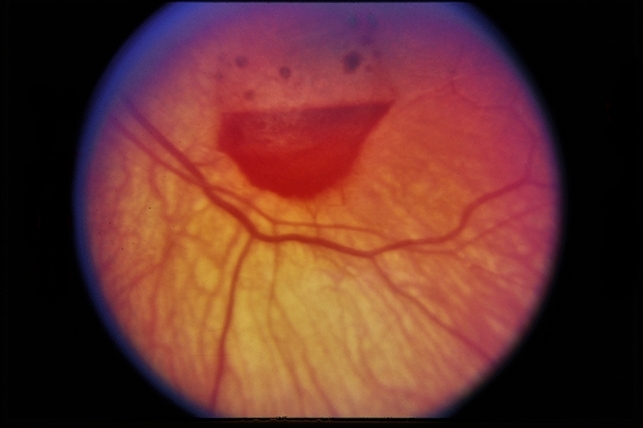
On the second postoperative day, he underwent an ophthalmological examination of the right eye, which showed visual acuity of 6/20 without correction, normal ocular tone, a normal anterior segment, and on the fundus examination, a stage 2 intravitreal hemorrhage organized inferiorly, with a flat retina superiorly.
A B-mode ocular ultrasound confirmed the intravitreal hemorrhage and did not find an associated retinal detachment. The examination of the left eye was unremarkable.
Given the cerebral and ocular involvement, the diagnosis of Terson syndrome was made.
Terson Syndrome DISEASE entity
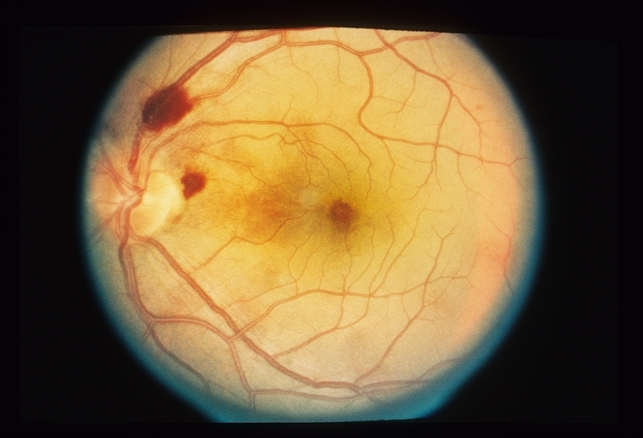
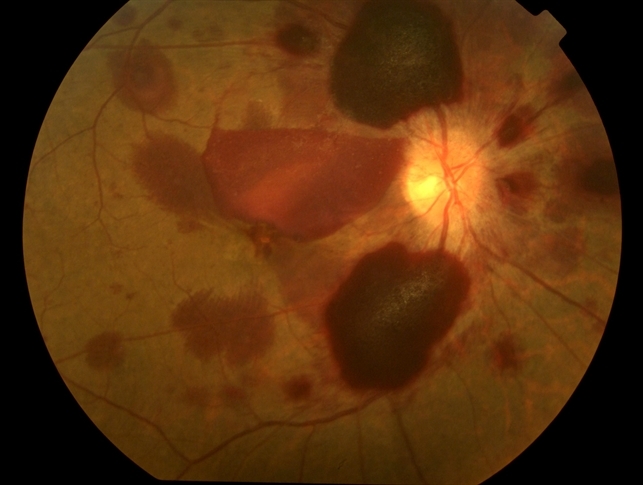
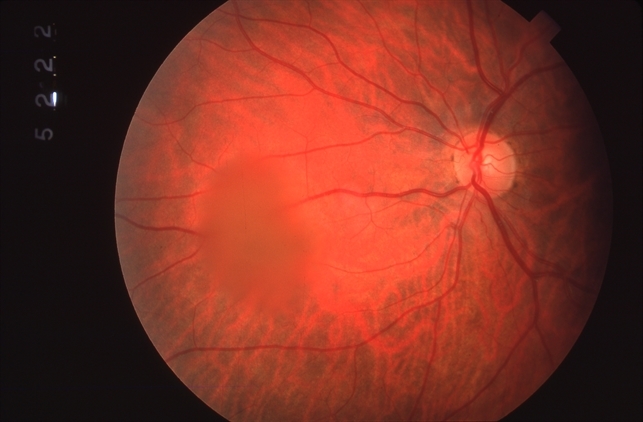
Terson syndrome is now recognized as an intraocular hemorrhage associated with SAH, intracerebral hemorrhage, or traumatic brain injury. Hemorrhage may be present in the vitreous, sub-hyaloid, subretinal space, or beneath the internal limiting membrane.
Vitreous hemorrhage associated with subarachnoid hemorrhage (SAH) was first described by German ophthalmologist Moritz Litten in 1881 and, then in 1900 by French ophthalmologist Albert Terson.
Terson syndrome has been reported in 8-19.3% of SAH, 9.1% of intracerebral hemorrhages, and 3.1% of traumatic brain injuries. 5.5% of vitreous hemorrhages not caused by diabetes or trauma are caused by Terson syndrome.
It usually occurs in adults but has been reported in children as young as 7 months. It can be unilateral or bilateral.
MANAGEMENT of Terson Syndrome
Intraocular hemorrhage frequently resolves spontaneously. Vision loss is usually reversible but permanent impairment of vision can occur. It has been reported that about 50% of vitreous hemorrhages do not resolve after 19 months.
There is no consensus on the optimal timing for vitrectomy in Terson syndrome. Vitreous hemorrhage can be observed for up to 3 months before considering pars plana vitrectomy.
This is supported by a study of 36 eyes with Terson syndrome in which eyes that were operated on within 90 days of the occurrence of VH had better final VA than eyes that were operated on after 90 days.
If the hemorrhage is bilateral or occurs in a young child at risk of amblyopia, one may proceed with surgery sooner. Augsten recommends operating within 4-8 weeks after the injury in patients with bilateral Terson syndrome.
In another study on PPV for Terson syndrome, 96% of patients had rapid visual improvement and 81% had better than 20/30 vision. In a series of 15 eyes that underwent PPV for VH, 93% had a final VA of 20/40 or better. ILM peeling has also been described in the surgical management of Terson syndrome.
Younger patients (<45 years old) who undergo PPV for Terson syndrome have better final visual acuity than older patients (>45 years old).
Studies have shown no difference in final visual acuity between patients who were conservatively managed and those who underwent PPV. However, visual recovery was more rapid in the vitrectomy group despite these patients having a denser vitreous hemorrhage.
Intravitreal TPA and gas have been used for recalcitrant Terson syndrome.
One patient with Terson syndrome and premacular subhyaloid hemorrhage was treated with Nd-YAG to puncture the posterior hyaloid face to allow drainage of blood into the vitreous. VA improved from 20/400 before treatment to 20/20 one month after treatment.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
REFERENCES
- AAO One Network Images. one.aao.org/images/terson-syndrome
- Czorlich P, Skevas C, Knospe V, et al. Terson syndrome in subarachnoid hemorrhage, intracerebral hemorrhage, and traumatic brain injury. Neurosurg Rev. Epub 2014 Aug 31.
- Skevas C, Czorlich P,Knospe V, et al. Terson’s syndrome–rate and surgical approach in patients with subarachnoid hemorrhage: a prospective interdisciplinary study. Ophthalmology. 2014 Aug;121(8):1628-33.
- Iuliano L, Fogliato G, Codenotti M. Intrasurgical imaging of subinternal limiting membrane blood diffusion in terson syndrome. Case Rep Ophthalmol Med. 2014;2014:689793.
- Michalewska Z, Michalewski J, Nawrocki J. Possible methods of blood entrance in Terson syndrome. Ophthalmic Surg Lasers Imaging. 2010 Nov-Dec;41 Suppl:S42-9.
- Morris R., Kuhn F., and Witherspoon C.D.: Hemorrhagic macular cysts. Ophthalmology 1994; 101: 1.

{kind=link}