
CASE REPORT
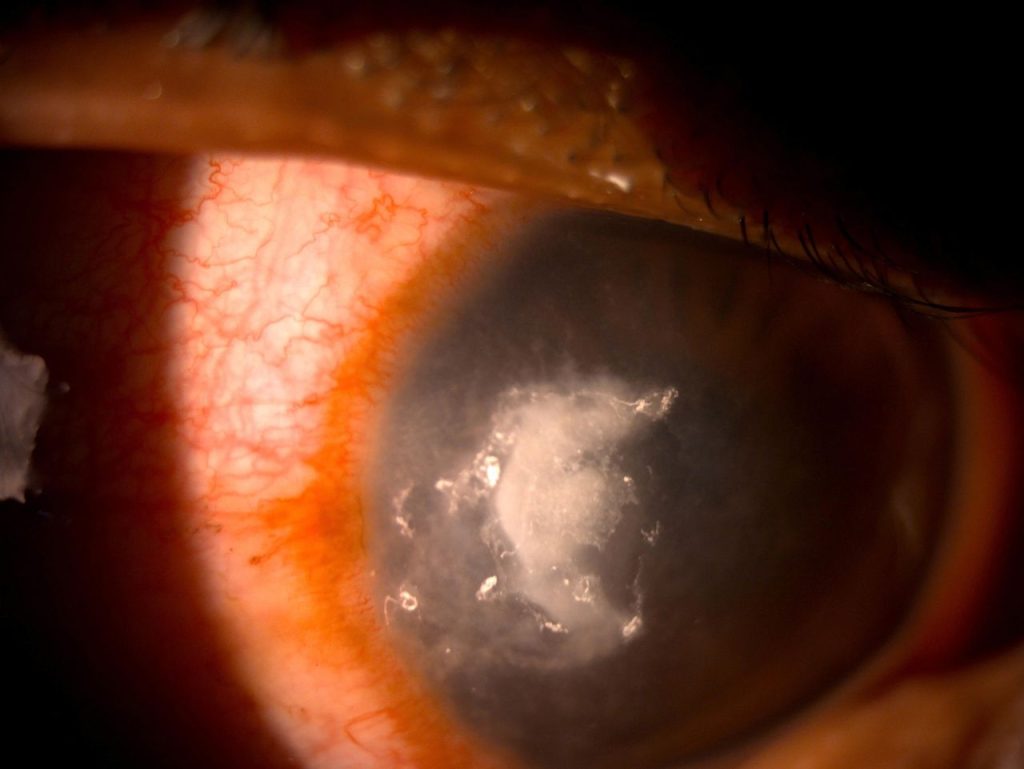
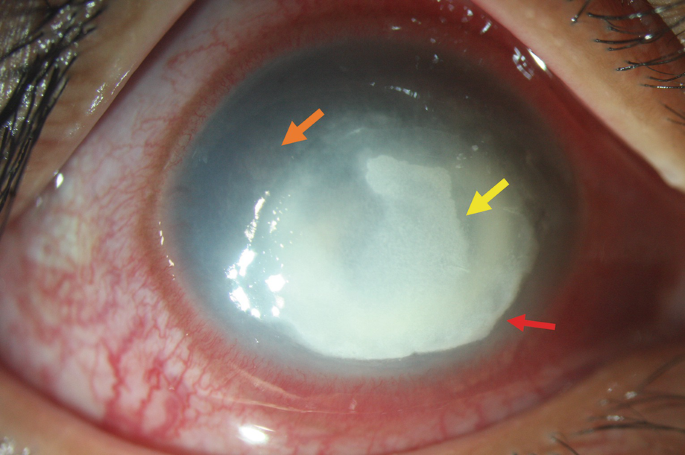
A 54- year- old male presented to a clinic with a PUK in the right eye. Systemic investigations were performed to rule out associated collagen vascular disorders. A microbiological examination of corneal scrapings was performed to rule out secondary infection which revealed gram-positive cocci on Gram stain.

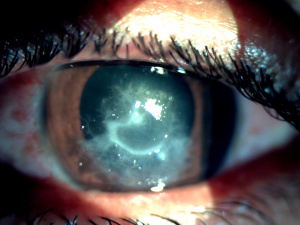
There was no growth of any organism on culture. Topical vancomycin 5% and ciprofloxacin 0.3% were started initially. On regular follow-up, there was a worsening of clinical signs. Topical and oral corticosteroids were further added.
Due to the progressive worsening of infiltrate size and corneal perforation, therapeutic penetrating keratoplasty was performed. Pythium insidiosum (confirmed by DNA sequencing and zoospore formation) was grown from the excised corneal button and the histopathology revealed filaments suggestive of Pythium species.
Pythium keratitis entity
Keratitis is caused by the fungus-like aquatic oomycete Pythium insidiosum. Pythium keratitis is a relatively rare form of keratitis but its potential to cause blinding manifestations in the eye, makes it an important cause.
It is most frequently misdiagnosed as fungal keratitis. It belongs to the Phylum Straminipila, Class Oomycetes, Order Pythiales, and Family Pythiaceae.
Pythium is found in tropical, subtropical, and temperate climates. The majority of the early reports were from Thailand. The first case of ocular pythiosis was reported in 1988 and since then numerous cases have been reported from all over the world.
Despite the omnipresence of this organism, ocular pythiosis cases have been underdiagnosed and less frequently reported. Apart from ocular disease, subcutaneous, vascular, and systemic pythiosis have been documented in the literature.
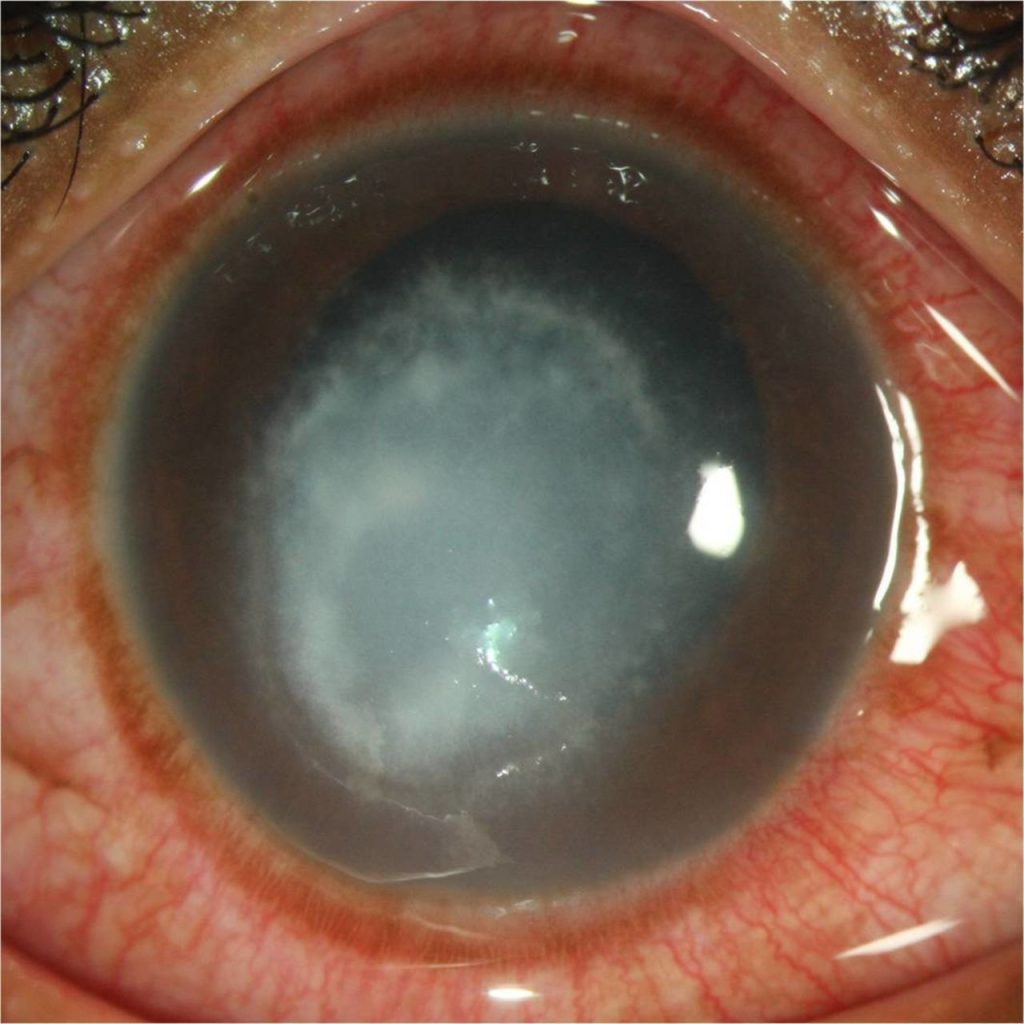
Many studies on Pythium keratitis from southern India have been documented. Two forms of the organism are known: the hyphate form with right-angle branching and broad filaments, and the infective form biflagellate zoospore in aquatic environments.
management of Pythium keratitis
Pythium keratitis is not very good firstly due to delay in diagnosis and secondly because of the dearth of management options. The remission of disease by medical therapy alone is questionable.
As already discussed, P. insidiosum is refractory to antifungal therapy. However few cases have been seen to respond to 1% itraconazole. In vitro studies have shown varied success with antimicrobials acting on protein synthesis inhibition. In particular, macrolides and tetracyclines have shown synergistic activity.
Medical Management of Pythium keratitis
Antibacterial drugs like azithromycin and minocycline have shown success in the management of Pythium keratitis. A triple regimen consisting of topical linezolid 0.2% hourly, topical azithromycin 1% hourly, and oral azithromycin 500mg for 3 days each week till expanding lesions resolve has been proven beneficial.
But this therapy worked only in less severe cases (<6mm). Other combinations like that of topical and oral azithromycin and topical voriconazole, a combination of topical minocycline ointment four times daily, hourly chloramphenicol drops and oral linezolid 1200 mg BD, and a combination of oral doxycycline and clindamycin and topical azithromycin have also been used with partial success.
Β-glucan inhibitors like caspofungin have been tried but are inconclusive. Another agent, mefenoxam, an RNA synthesis inhibitor, has shown some promise in animal experiments. Debulking of infectious load by scraping can be beneficial but caution should be executed for the risk of perforation in severe cases.
Surgical Management of Pythium keratitis
Early penetrating keratoplasty in diagnosed cases has been believed to be the gold standard treatment. A clear margin of 1 mm incorporating the reticular expanding lesions is advocated. Thorough anterior chamber wash should be accompanied to leave no residual focus of infection otherwise recurrence is a rule.
Adjunctive modalities have been used to decrease recurrence. These include single-cycle cryotherapy with a retinal probe at the graft host junction. In patients with scleral involvement, 99.9% absolute alcohol should be applied beyond cryo marks extending to the posterior limit of the infected sclera for 20 seconds.
Evisceration or enucleation may be required in severe infection with diffuse scleritis or endophthalmitis. Isolated reports of vaccines containing P. Insidiosum antigen (PIA) used to decrease post-keratoplasty infection recurrence have been noted. But the success of this therapy is not documented and needs larger study validation.
Monitoring and Follow-up
Daily monitoring of these cases is warranted for timely intervention. The rapidly progressive and aggressive nature of the pathogen can lead to a sudden worsening in a matter of a few days. There is a more than 50% recurrence reported even after timely surgical intervention by penetrating keratoplasty and as early as within two weeks.
Careful evaluation of graft clarity and particularly graft host junction should be done. Any new infiltrate or anterior chamber exudation should be considered serious. These patients may need prompt regrafting with additive therapies in the form of cryo or alcohol treatment as described.
Severe cases, suspected orbital infections, and large scleral involvement should undergo imaging to rule out chances of cavernous sinus thrombosis.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian J Ophthalmol. 2021 May;69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. PMID: 33913840.
- Virgile R, Perry HD, Pardanani B, et al. Human infectious corneal ulcer caused by Pythium insidiosum. Cornea. 1993;12:81–83.
- Triscott JA, Weedon D, Cabana E. Human subcutaneous pythiosis. J Cutan Pathol 1993;20:267-71
- Sudjaritruk T, Sirisanthana V. Successful treatment of a child with vascular pythiosis. BMC Infect Dis 2011;11:33.
- Reanpang T, Orrapin S, Orrapin S, Arworn S, Kattipatanapong T, Srisuwan T, et al. Vascular pythiosis of the lower extremity in Northern Thailand: Ten years’ experience. Int J Low Extrem Wounds 2015;14:245-50
- Smith F. The pathology of bursattee. Vet J 1884;19:16-7.
- Thanathanee O, Enkvetchakul O, Rangsin R, Waraasawapati S, Samerpitak K, Suwan-Apichon O, et al. Outbreak of Pythium keratitis during rainy season: A case series. Cornea 2013;32:199-204.

{kind=link}