
Gyrate Atrophy case report
28-year-old man consulting for a progressive fall of visual acuity with hemeralopia. Eye fundoscopy showed regions of confluent rounded chorioretinal atrophy.


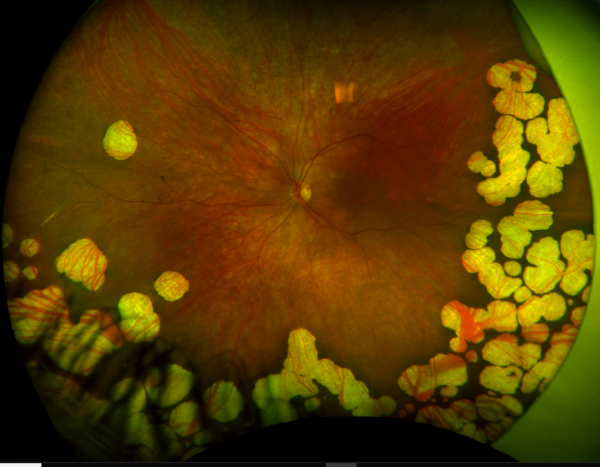
Widefield fundus photography showing early gyrate atrophy with characteristic scattered chorioretinal lesions in the periphery. An important differential is paving stone degeneration, which however usually does not extend posteriorly beyond the equator.
The visual field and retinal angiography were altered. A high level of plasma ornithine (629 nmol/mL) was detected and a diagnosis of gyrate atrophy of the retina and choroid was made.
Disease
Gyrate Atrophy of the choroida and the retina is a rare autosomal recessive retinal dystrophy characterized by progressive chorioretinal degeneration, early cataract formation, and myopia.
It is caused by a deficiency in the enzyme ornithine aminotransferase (OAT), which results in a 10- to 20-fold increase in plasma ornithine concentrations.
Patients classically present in the first decade of life with nyctalopia, with fundus exam revealing characteristic circular patches of chorioretinal atrophy distributed in the peripheral fundus.
As the disease progresses, the atrophic lesions coalesce and advance centripetally toward the posterior pole, correlating with progressive loss of peripheral vision. Macular involvement occurs late in the disease.
Histology
Histology of atrophic lesions shows complete absence of outer retina, RPE, Choriocapillaris, and many of the medium and large choroidal vessels.
Directly adjacent to the atrophic areas, there is focal photoreceptor atrophy with underlying hyperplastic RPE.
Genetics
Gyrate Atrophy is due to various mutations in the OAT gene, which is found on chromosome 10q26. Inheritance is autosomal recessive. More than 50 variants have been identified, with missense mutations occurring most frequently.
These mutations lead to truncation of the enzyme ornithine aminotransferase, causing protein degradation.
A subset of patients carries a genetic variant that is favorably responsive to supplementation with co-factor pyridoxine (vitamin B6), which has been shown to partially restore the function of the OAT enzyme.

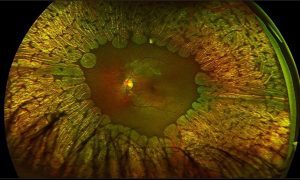
Widefield fundus photography showing an advanced case of gyrate atrophy. Previously circular atrophic lesions have coalesced to form a large confluent area of atrophy with islands of the preserved retina and late preservation of the macula. Note the hyperpigmentation of the macula.
Pathophysiology
The underlying biochemical defect of gyrate atrophy is in ornithine aminotransferase (OAT), a vitamin B6-dependent mitochondrial matrix enzyme.
OAT catalyzes the conversion of L-ornithine, a non-proteinaceous amino acid, to proline and glutamic acid, serving in the exchange of molecules between the urea and Krebs’s cycle.
OAT plays a critical role in cellular detoxification by disposing of ornithine derived from dietary arginine. A deficiency of OAT thus leads to ornithine accumulation, with levels 10-to 20-fold above normal.
The mechanism by which a deficiency of OAT and the consequent accumulation of ornithine lead to the chorioretinal degeneration is not fully understood.
Possibilities include a direct toxic effect of the accumulated ornithine or one of its metabolites.
![]() Indeed,
Indeed,
animal models have shown that intravitreal injections of ornithine induced the development of degeneration similar to that observed in gyrate atrophy.
It has been suggested that the retinal pigment epithelium (RPE) is the site of the initial insult due to its reliance on OAT activity for metabolic functions.
RPE injury then leads to a breakdown of the outer blood-retinal barrier causing photoreceptor cell exposure to toxic agents from choroidal circulation.
Historically,
other theories proposed that damage to the retina might occur secondary to high ornithine concentrations inhibiting creatine biosynthesis, a key agent in cellular energy storage.
creatine supplementation has not been proven to slow the retinal disease and its role in pathogenesis remains unclear.

Metabolism of ornithine as related to gyrate atrophy.
Diagnosis
Gyrate Atrophy of the choroid and the retina is largely a clinical diagnosis based on history and examination. Elevated levels of systemic ornithine and genetic sequencing confirm the diagnosis.
Take a break and read about retinal imaging by your smartphone. then continue with gyrate atrophy symptoms..
Symptoms
Patients initially present with myopia and nyctalopia that begins in late childhood. As the disease progresses in the second decade of life, patients report progressive loss of peripheral vision.
Visually significant posterior subcapsular cataracts develop early in virtually all patients, frequently by the second decade of life. Vision loss secondary to cystoid macular edema is common.
Exam Findings
Fundus examination early in the disease course shows bilateral patchy, sharply demarcated circular areas of chorioretinal atrophy with hyperpigmented margins in the mid to far periphery.
Typically,
during the second decade of life, the peripheral atrophic lesions coalesce and spread toward the posterior pole, forming a confluent lesion with a scalloped border at the junction of healthy and diseased retinal pigment epithelium.
The remaining healthy RPE in uninvolved areas is hyperpigmented, distinguishing this disease from Choroideremia.
The macula and thus central vision are spared until late in the disease course, often preserved into the fourth or fifth decade of life. In a study of 21 patients with long-term follow-up and serial fundus angiography, 8 (38%) had a macular distribution of the atrophy.
Systemic Features
Non-ocular findings include mild cognitive impairment, delayed language development, and speech defects. MR imaging has shown up to 70% have premature atrophic changes in the brain.
Other findings include thin, sparse hair and muscular atrophy. There is progressive atrophy of skeletal muscle fibers (specifically type II) both radiographically and histologically, although most patients deny muscular symptoms.
Laboratory Tests
Levels of ornithine have been reported to be 10 to 20 times higher than normal in plasma, urine, spinal fluid, and aqueous humor. Gene sequencing analysis is helpful in confirming and identifying the allelic variant.
Other biochemical abnormalities include hypo glutamic acidemia, hypolysenima, hypoglutanemia, and hyperammonemia.
Fundus Photography
Serial fundus photography, especially wide-field Retinal imaging, is useful in monitoring the progression of the disease. In a study of two related patients with an unrestricted diet and photos taken 24 months apart.
younger age and smaller lesion sizes at baseline were associated with a significantly faster rate of chorioretinal degeneration.

Fundus autofluorescence of a patient with early gyrate atrophy showing temporal peripheral clusters of diminished autofluorescence, which correlates with chorioretinal atrophy seen on retinal photograph. Note the thinly demarcated hyperautofluorescent perimeter.
Fundus Autofluorescence
Depending on the disease severity, fundus autofluorescence shows either focal or confluent areas of absent autofluorescence, which corresponds with the areas of chorioretinal atrophy seen on the fundus exam.
These atrophic lesions are commonly surrounded by a sharply demarcated hyperautofluorescent perimeter. The remaining unaffected area, which typically includes the macula, is normal.

SD-OCT in a patient with gyrate atrophy demonstrating intraretinal hyperreflective cavities.
Optical Coherence Tomography
The IS/OS junction is typically preserved in the regions where the autofluorescence signal is normal or increased. In the periphery, extensive loss of IS/OS junction, RPE, and inner choroid reflectivity, accompanied by significant thinning of both inner and outer retina are often observed concurrently.
Cystoid macular edema is frequent, presumed to be due to impairment of the blood-retinal barrier. The largest case series with SD-OCT imaging showed all 7 (100%) patients were found to have multiple intraretinal cystoid changes and thickening of the fovea.
,
it is important to note whether there is a petaloid leak at the macula in the late phase of the fundus fluorescein angiogram. In the presence of vertical tissue bridges, hypo reflective spaces in the retina on SD-OCT.
the term foveschisis is used. Macular hole and epiretinal membrane are other possible macular involvement in the gyrate atrophy of the choroid and the retina.
Other findings in advanced disease can include deposits of retinal gliosis, outer retinal tabulation, and choroidal neovascularization.
Electroretinography (ERG)
ERG abnormalities are present at an early stage of the disease, with impaired rod and cone responses, ultimately progressing to a completely extinguished response.
THE Median ERG half-life is 16.0 years (standard combined response) and 10.7 years (flicker response).
Differential Diagnosis
- Choroideremia
- Retinitis Pigmentosa
- Myopic Degeneration
- Cobblestone Degeneration
- Diffuse Choriocapillaris Atrophy
- Multifocal choroiditis
Management
There is no curative regimen for gyrate atrophy. Lowering the elevated systemic ornithine is presumed to slow disease progression, but the utility of such measures is difficult to prove due to the disease’s rarity and slow rate of change.
Refraction and low vision aid should be tried to improve vision and associated quality of life. Examination of the fundus of family members is also important.
Whereas,
small case series and anecdotal evidence on human subjects suggest that correction of hyperornithinemia seems to be beneficial, animal models have been more definitive in providing histopathologic evidence that early treatment alters the natural history of the disease:
- Low-protein, Arginine-Restricted diet
- Vitamin B6 Supplementation
- Creatine Supplementation
Cystoid Macular Edema (CME)
There is no consensus regarding the treatment of CME. Single case reports have shown improvement with a sub-tenon injection of triamcinolone acetonide, dexamethasone implantation, intravitreal bevacizumab, and topical NSAIDs.
There is no clear data regarding the utility of systemic carbonic anhydrase inhibitors. One study has shown improvement in two patients with a low-protein, arginine-restricted diet.
As mentioned earlier,
if is important to differentiate CME from foveschisis which doe not cause a leak of fluorescein on fluorescein angiogram (FA). Typically, CME with peraloid leak on FA responds better to intravitreal/periocular steroid injections,
whereas for foveschisis dorzolamide drops and/or acetazolamide tablets are preferred.
Cataract Surgery
Cataracts typically occur by the second decade of life, frequently requiring surgical intervention by the third decade of life. Posterior subcapsular and posterior sutural cataracts are most common.
More about Choroidal Osteoma, Retinitis Pigmentosa
Prognosis
Vision loss is slow and progressive. Considerable variability is observed both in the age at which visual acuities begin to decrease and the age at which visual acuities reach 20/200.
Without cataract surgery, the percentage of eyes with acuity 20/200 or worse has been reported as 37% at age 30 and 64% at age 40. In patients with a history of cataract surgery,
this rate decreased to 20% at age 40. The median visual field half-life of 17.0 years for static perimetry and 11.4 years for kinetic perimetry.
Future Therapeutics
There are no known ongoing clinical trials. As with many of the inherited retinal dystrophies, gene therapy is a promising emerging technology.
would you have the interest to take smartphone slit-lamp photography ?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera.

References
- Tripathy K, Chawla R, Sharma YR, Gogia V. Ultrawide field fluorescein angiogram in a family with gyrate atrophy and foveoschisis. Oman J Ophthalmol. 2016;9(2):104–106. doi:10.4103/0974-620X.184529
- Takki K, Milton R. The Natural History of Gyrate Atrophy of the Choroid and Retina. Ophthalmology. 1981 Apr;88(4):292-301.
- Valle, D., Simell, O. The hyperornithinemias. In: Scriver, C. R.; Beaudet, A. L.; Sly, W. S.; Valle, D. (eds.): The Metabolic and Molecular Bases of Inherited Disease. Vol. II. (8th ed.) New York: McGraw-Hill (pub.) 2001. Pp. 1857-1895.
- Simell, O., Takki, K. Raised plasma ornithine and gyrate atrophy of the choroid and retina. Lancet 301: 1031-1033, 1973
- Brody, L. C., Mitchell, G. A., Obie, C., Michaud, J., Steel, G., Fontaine, G., Robert, M.-F., Sipila, I., Kaiser-Kupfer, M., Valle, D. Ornithine delta-aminotransferase mutations in gyrate atrophy: allelic heterogeneity and functional consequences. J. Biol. Chem. 267: 3302-3307, 1992
- Valle D, Simell O. In: The Metabolic and Molecular Bases of Inherited Disease. Scriver C, Beaudet A, Sly W, Valle D, editors. New York: McGraw–Hill; 1995. pp. 1147–1185
- Montioli R1, Desbats MA2, Grottelli S3, Doimo M2, Bellezza I3, Borri Voltattorni C1, Salviati L4, Cellini B5. Molecular and cellular basis of ornithine δ-aminotransferase deficiency caused by the V332M mutation associated with gyrate atrophy of the choroid and retina. Ophthalmic Genet. 2018 Aug;39(4):512-516.
- Mashima YG, Weleber RG, Kennaway NG, Inana G. Genotype-phenotype correlation of a pyridoxine-responsive form of gyrate atrophy. Ophthalmic Genet. 1999 Dec;20(4):219-24.
- Cui X, Jauregui R, Park KS, Tsang SH. Multimodal characterization of a novel mutation causing vitamin B6-responsive gyrate atrophy. Ophthalmic Genet. 2018 Aug;39(4):512-516.
- Shih VE, Mandell R, Berson EL.Pyridoxine effects on ornithine ketoacid transaminase activity in fibroblasts from carriers of two forms of gyrate atrophy of the choroid and retina. Am J Hum Genet. 1988 Dec;43(6):929-33.
- ODonnell JJ, Sandman RP, Martin SR (1978) Gyrate atrophy of the retina: inborn error of L-ornithine: 2-oxoacid aminotransferase. Science 200:200–201
- Volpe P, Sawamura R, Strecker HJ (1969) Control of ornithine delta-transaminase in rat liver and kidney. J Biol Chem 244:719–726

{kind=link}