
Case Study
A 28-year-old woman presented with an acute onset of blurred vision and a paracentral scotoma in her left eye for five days. She also reported intermittent headaches and recent difficulty hearing in her right ear.


There was no history of autoimmune disease. Best-corrected visual acuity was 20/25 in the right eye and 20/40 in the left.
Anterior segment examination was unremarkable, and there was no relative afferent pupillary defect.
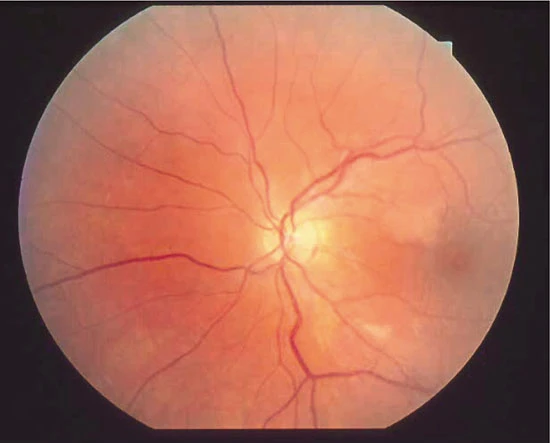
Dilated fundus examination of the left eye revealed multiple branch retinal artery occlusions (BRAOs) with subtle retinal whitening along the superotemporal arcade.
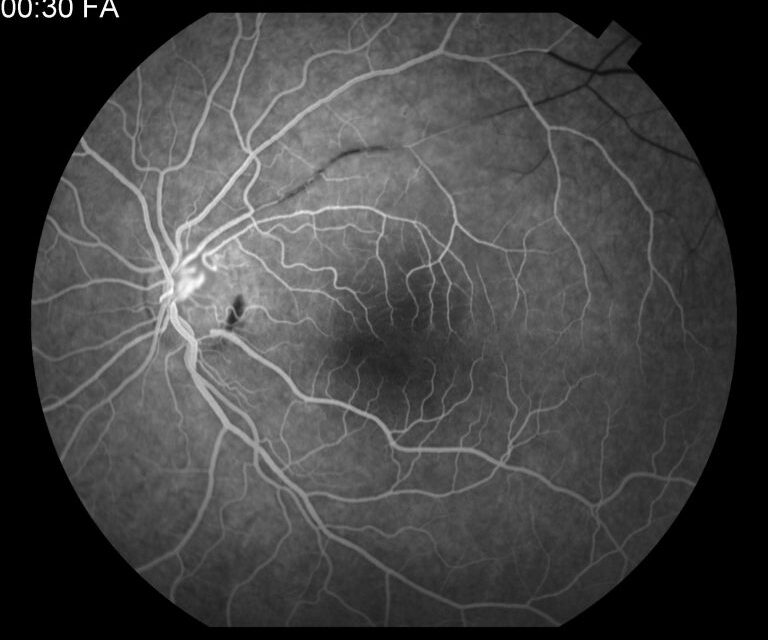
The right eye showed mild arterial wall hyperfluorescence without obvious occlusion. Fluorescein angiography (FA) demonstrated segmental arterial wall hyperfluorescence and areas of nonperfusion consistent with BRAOs.
Optical coherence tomography (OCT) showed inner retinal hyperreflectivity corresponding to areas of ischemia.
Brain magnetic resonance imaging (MRI) revealed characteristic corpus callosum lesions. Audiometry confirmed low-frequency sensorineural hearing loss.
A diagnosis of Susac syndrome was established. The patient was started on high-dose systemic corticosteroids followed by immunosuppressive therapy.
Disease Entity
Susac syndrome is a rare autoimmune endotheliopathy characterized by the clinical triad of:
-
Branch retinal artery occlusions (BRAOs)
-
Encephalopathy
-
Sensorineural hearing loss
The condition primarily affects precapillary arterioles of the brain, retina, and inner ear. Although the complete triad is classic, many patients present initially with isolated ocular findings, particularly BRAOs.
Retinal artery involvement is often the first manifestation and may precede neurologic or audiologic symptoms. The disease predominantly affects young women and may follow a relapsing-remitting or monophasic course.
Early recognition of retinal findings is critical, as prompt immunosuppressive therapy can prevent permanent neurologic and auditory deficits.
Pathophysiology
Susac syndrome is believed to be an autoimmune-mediated microangiopathy targeting endothelial cells of small arterioles. Anti-endothelial cell antibodies have been detected in some patients, supporting an immune-mediated process.
Histopathologic studies demonstrate microvascular occlusion due to endothelial swelling, basement membrane thickening, and luminal narrowing.
Unlike embolic retinal artery occlusion, the occlusion in Susac syndrome is inflammatory rather than thromboembolic.
In the retina, arteriolar involvement leads to focal ischemia in the inner retinal layers, corresponding to BRAOs. In the brain, microinfarctions predominantly affect the corpus callosum.
In the cochlea, ischemia of the apical turn results in low-frequency hearing loss.
The disease process is segmental and multifocal, explaining the patchy and recurrent nature of vascular occlusions.
Epidemiology
Susac syndrome is rare, with several hundred cases reported worldwide. It most commonly affects women between 20 and 40 years of age, with a female-to-male ratio of approximately 3:1.
The condition is not associated with a specific racial predilection. The disease course varies from self-limited monophasic illness lasting 1–3 years to chronic relapsing disease.
Because early symptoms may be nonspecific, diagnosis is often delayed.
Clinical Features
Ocular manifestations primarily consist of branch retinal artery occlusions.
Symptoms may include:
-
Acute or subacute visual field defects
-
Paracentral scotomas
-
Blurred vision
-
Photopsias (occasionally)
Visual acuity may be preserved if the macula is spared.
Neurologic features include:
-
Headache
-
Cognitive dysfunction
-
Confusion
-
Behavioral changes
-
Focal neurologic deficits
Audiologic symptoms include:
-
Sudden or fluctuating hearing loss
-
Tinnitus
-
Vertigo
The full triad may not be present at initial presentation. Retinal findings may precede neurologic symptoms by weeks to months.

Examination Findings
Anterior segment examination is typically normal.
Fundus findings include:
-
Multiple BRAOs
-
Retinal whitening along affected arterioles
-
Arterial wall plaques (Gass plaques)
-
Minimal or absent embolic material
Gass plaques represent focal arterial wall hyperfluorescence rather than emboli.
Fluorescein Angiography (FA)
-
Segmental arterial wall hyperfluorescence
-
Areas of branch retinal artery nonperfusion
-
Minimal leakage
-
Arteriolar wall staining
Optical Coherence Tomography (OCT)
-
Inner retinal hyperreflectivity in acute phase
-
Subsequent inner retinal thinning in chronic stage
Optical Coherence Tomography Angiography (OCTA)
-
Focal capillary nonperfusion corresponding to BRAOs
Neuroimaging
Brain MRI classically shows:
-
T2 hyperintense lesions in the corpus callosum
-
“Snowball” lesions are centrally located within the callosal body
-
Lesions in white matter and deep gray structures
Audiologic Testing
-
Low-frequency sensorineural hearing loss
-
Reduced speech discrimination
Differential Diagnosis
The differential diagnosis includes:
-
Embolic branch retinal artery occlusion
-
Central nervous system vasculitis
-
Multiple sclerosis
-
Cogan syndrome
-
Antiphospholipid antibody syndrome
-
Systemic lupus erythematosus
Embolic BRAO typically presents in older patients with vascular risk factors and identifiable emboli.
Multiple sclerosis may present with white matter lesions but lacks retinal arterial occlusions.
Cogan syndrome includes interstitial keratitis rather than retinal artery involvement.
A comprehensive systemic evaluation is necessary to exclude alternative causes of retinal and neurologic ischemia.
Diagnosis
Diagnosis is clinical, supported by imaging and audiologic testing.
Diagnostic criteria generally include:
-
Evidence of BRAOs
-
Characteristic brain MRI findings
-
Sensorineural hearing loss
The presence of two components of the triad with supportive imaging is often sufficient for diagnosis.
Laboratory testing is typically nonspecific but may be performed to exclude other autoimmune or vasculitic conditions.
Early ophthalmologic recognition plays a pivotal role in initiating systemic workup.
Management
Susac syndrome requires aggressive immunosuppressive therapy to prevent irreversible neurologic and auditory damage.
Treatment strategies may include:
-
High-dose intravenous corticosteroids
-
Oral corticosteroid taper
-
Intravenous immunoglobulin (IVIG)
-
Mycophenolate mofetil
-
Azathioprine
-
Cyclophosphamide
-
Rituximab
Combination therapy is often recommended in moderate to severe cases.
Antiplatelet agents are sometimes used, although the primary pathology is inflammatory rather than thrombotic.
Close multidisciplinary collaboration among ophthalmology, neurology, and otolaryngology is essential.
Monitoring includes serial visual fields, OCT, brain MRI, and audiometry.
Prognosis
The prognosis varies depending on disease severity and treatment timing.
Visual outcomes are generally favorable if macular involvement is limited. However, permanent visual field defects may persist.
Neurologic deficits may improve with treatment but can leave residual cognitive impairment.
Hearing loss is often irreversible, particularly if treatment is delayed.
Early and sustained immunosuppression improves long-term outcomes and reduces relapse risk.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Susac JO, Hardman JM, Selhorst JB. Microangiopathy of the brain and retina. Neurology. 1979;29(3):313–316.
-
Egan RA, Hills WL, Susac JO. Gass plaques and fluorescein angiographic findings in Susac syndrome. Retina. 2010;30(1):131–138.
-
Dörr J, Krautwald S, Wildemann B, et al. Characteristics of Susac syndrome: a review of all reported cases. Nat Rev Neurol. 2013;9(6):307–316.
-
Jarius S, Neumayer B, Wandinger KP, et al. Anti-endothelial serum antibodies in Susac syndrome. J Neurol Sci. 2009;285(1-2):259–262.

{kind=link}