
Case Study
A 17-year-old male was referred for evaluation of an incidental retinal vascular lesion detected during routine examination.


He was asymptomatic, with best-corrected visual acuity of 20/20 in both eyes. There was no history of ocular trauma, systemic illness, or visual complaints.
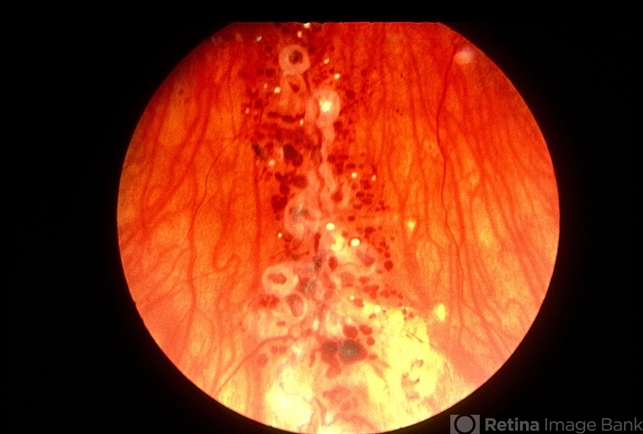
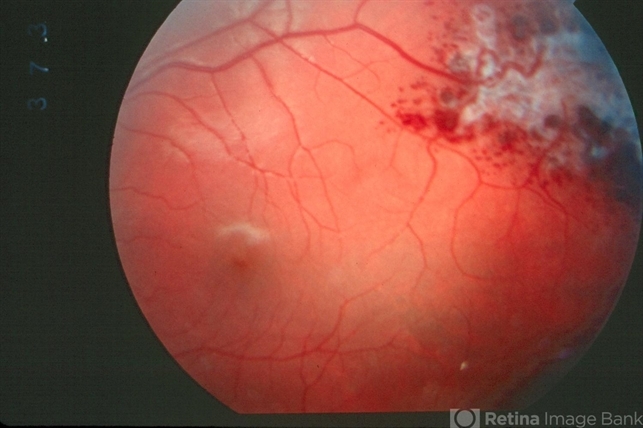
Fundus examination of the left eye revealed a cluster of saccular, dark red vascular dilations resembling a “bunch of grapes” along the superotemporal arcade.
The lesion appeared intraretinal, with overlying glial tissue and minimal surrounding exudation. The right eye was normal.
Fluorescein angiography (FA) demonstrated slow filling of the saccular aneurysmal spaces with delayed venous phase fluorescence and characteristic plasma–erythrocyte layering, producing a “fluorescence capping” appearance.
There was no leakage in the late phases. Optical coherence tomography (OCT) showed cystic, hyporeflective intraretinal spaces corresponding to the vascular cavities without subretinal fluid.
Neuroimaging was performed to exclude associated cerebral vascular malformations and was unremarkable.
A diagnosis of retinal cavernous hemangioma was made. The patient was managed conservatively with periodic observation.
Disease Entity
Retinal cavernous hemangioma is a rare, benign congenital vascular hamartoma characterized by clusters of thin-walled, saccular intraretinal vascular dilations.
It is typically unilateral and non-progressive, although rare bilateral cases have been described.
The lesion consists of grape-like aneurysmal vascular sacs filled with sluggish blood flow. It may occur sporadically or as part of a systemic vascular disorder, particularly familial cerebral cavernous malformation syndrome.
Retinal cavernous hemangioma is distinct from retinal capillary hemangioblastoma and other retinal vascular tumors in its clinical appearance, angiographic behavior, and natural history.
Pathophysiology
Retinal cavernous hemangioma is considered a congenital vascular malformation rather than a true neoplasm.
It arises from developmental anomalies of the retinal vasculature, resulting in clusters of dilated, thin-walled vascular channels within the inner retina.
Histopathologic studies demonstrate endothelial-lined vascular spaces separated by minimal connective tissue stroma.
These vascular cavities contain slow-moving blood, which accounts for the characteristic plasma–erythrocyte separation seen on fluorescein angiography.
Unlike capillary hemangioblastomas, cavernous hemangiomas lack significant feeder vessels and typically do not exhibit active leakage or exudation. The absence of high-flow dynamics explains the generally stable clinical course.
In familial cases, mutations in genes associated with cerebral cavernous malformations (such as KRIT1/CCM1, CCM2, and PDCD10/CCM3) have been implicated.
These genetic associations underscore the importance of evaluating for central nervous system involvement in selected patients.
Epidemiology
Retinal cavernous hemangioma is rare, with most cases diagnosed in children or young adults. Both sexes are affected equally.
The lesion is usually unilateral and discovered incidentally during routine examination.
Familial cases may present earlier and can be associated with multiple systemic cavernous malformations, particularly in the brain.
There is no clear racial predilection. Because the condition is often asymptomatic and non-progressive, it may be underdiagnosed.
Clinical Features
Most patients are asymptomatic at presentation. When symptoms occur, they are typically related to complications such as vitreous hemorrhage.
Clinical features include:
-
Clustered, saccular, dark red intraretinal lesions
-
“Bunch of grapes” configuration
-
Location along the vascular arcades or in the peripheral retina
-
Overlying glial membrane in some cases
Visual acuity is usually preserved unless the lesion involves the macula or complications arise.
Occasionally, patients may present with:
-
Sudden visual decrease due to vitreous hemorrhage
-
Floaters
-
Rarely, epiretinal membrane formation
The lesion typically remains stable over time.
Examination Findings
Anterior segment examination is generally normal.
Fundus examination reveals:
-
Multiple saccular aneurysmal dilations
-
Dark red coloration due to stagnant blood
-
Intraretinal location, often in the inner retinal layers
-
Minimal surrounding exudation
An overlying gliotic membrane may be present, particularly in longstanding cases.
Fluorescein Angiography (FA)
FA findings are characteristic:
-
Delayed filling of aneurysmal sacs
-
Plasma–erythrocyte separation producing “fluorescence capping.”
-
Absence of significant leakage
-
No prominent feeder arteries
Optical Coherence Tomography (OCT)
-
Hyporeflective cystic spaces within the inner retina
-
Overlying hyperreflective membrane if gliosis is present
-
Typically, no subretinal fluid
Optical Coherence Tomography Angiography (OCTA)
-
Low-flow vascular channels
-
Limited flow signal due to sluggish circulation
Ultrasonography
-
Generally not required
-
May show localized retinal thickening in larger lesions
Neuroimaging (MRI of the brain) may be indicated when familial disease is suspected.
Differential Diagnosis
The differential diagnosis includes:
-
Retinal capillary hemangioblastoma
-
Coats disease
-
Retinal macroaneurysm
-
Racemose hemangioma (arteriovenous malformation)
-
Vasoproliferative tumor of the retina
Retinal capillary hemangioblastomas typically demonstrate prominent feeder vessels and significant exudation, often associated with von Hippel–Lindau disease.
Coats disease presents with telangiectatic vessels and extensive lipid exudation, primarily in young males.
Retinal macroaneurysms occur in older patients with systemic hypertension and involve larger arterioles.
Racemose hemangiomas show direct arteriovenous communications without capillary beds.
The absence of leakage and the characteristic angiographic “capping” phenomenon strongly favor cavernous hemangioma.
Diagnosis
Diagnosis is primarily clinical, supported by characteristic fluorescein angiographic findings.
Key diagnostic features include:
-
Grape-like clusters of saccular intraretinal aneurysms
-
Plasma–erythrocyte layering on FA
-
Absence of significant leakage
-
Minimal exudation
-
Stable clinical course
Systemic evaluation should be considered in:
-
Patients with a family history of cerebral vascular malformations
-
Multiple or bilateral lesions
-
Neurologic symptoms
Genetic counseling may be appropriate in familial cases.
Management
Most cases require no treatment.
Observation with periodic examination is appropriate for asymptomatic, stable lesions.
Intervention may be necessary in cases complicated by:
-
Recurrent vitreous hemorrhage
-
Significant visual impairment
-
Epiretinal membrane formation
Treatment options are limited and may include:
-
Pars plana vitrectomy for non-clearing vitreous hemorrhage
-
Surgical membrane peeling if tractional complications occur
Laser photocoagulation and anti-VEGF therapy are generally ineffective due to the low-flow nature of the lesion and absence of leakage.
Patients with associated cerebral cavernous malformations should be co-managed with neurology or neurosurgery.
Prognosis
The prognosis of retinal cavernous hemangioma is generally excellent.
Most lesions remain stable for years without a significant visual impact. Visual acuity is typically preserved unless complications arise.
Vitreous hemorrhage is the most common complication but it often resolves spontaneously. Recurrent hemorrhage may necessitate surgical intervention.
In familial cases, systemic prognosis depends on the presence and behavior of cerebral cavernous malformations.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
-
Shields CL, Shields JA. Intraocular Tumors: An Atlas and Textbook. 3rd ed. Wolters Kluwer; 2016.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Gass JDM. Stereoscopic Atlas of Macular Diseases: Diagnosis and Treatment. 4th ed. Mosby; 1997.
-
Witschel H, Font RL. Hemangioma of the retina. Am J Ophthalmol. 1976;82(4):519–531.
-
Singh AD, Shields CL, Shields JA. Retinal vascular tumors. Surv Ophthalmol. 2005;50(3):297–315.

{kind=link}