
Case Study
A 15-year-old previously healthy boy presented with sudden bilateral blurred vision and floaters for five days. He reported a mild headache and a recent viral-like illness two weeks earlier.

Best-corrected visual acuity was 20/60 in both eyes. Anterior segment examination revealed mild anterior chamber cells.
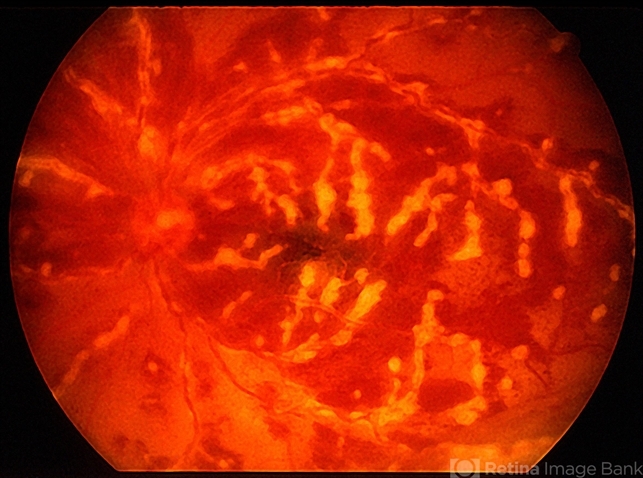
Dilated fundus examination demonstrated striking diffuse sheathing of retinal vessels resembling frosted tree branches, with extensive perivascular exudation, retinal hemorrhages, and mild optic disc edema.
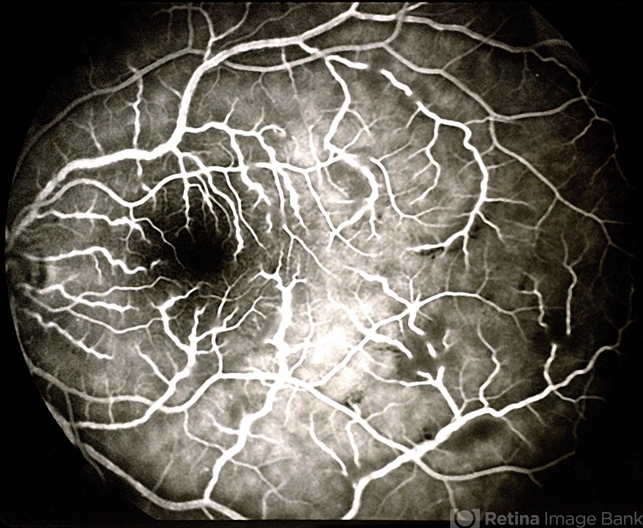
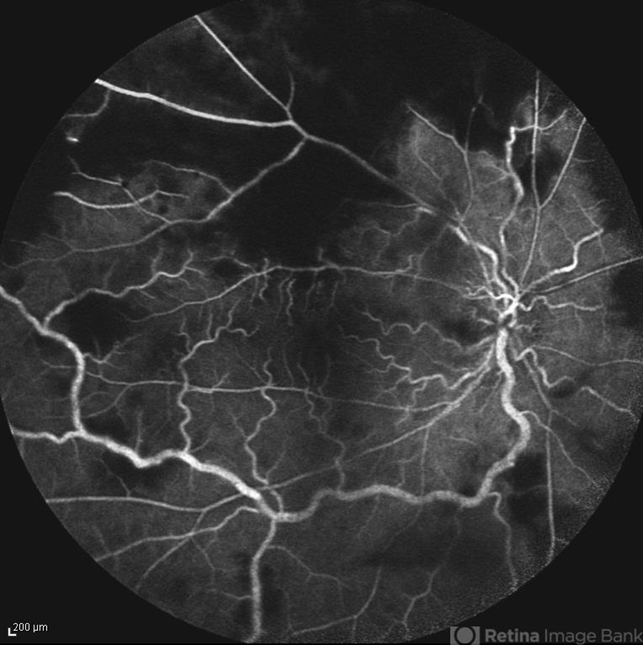
Fluorescein angiography (FA) revealed widespread vascular leakage from both arteries and veins, with staining of vessel walls and areas of capillary nonperfusion.
Optical coherence tomography (OCT) showed macular edema and hyperreflective inner retinal changes consistent with inflammatory involvement.
Laboratory workup excluded infectious causes such as cytomegalovirus and herpes viruses. A diagnosis of idiopathic frosted branch angiitis was established.
The patient was treated with high-dose systemic corticosteroids. Within two weeks, vascular sheathing and retinal inflammation markedly improved, and visual acuity recovered to 20/25 bilaterally over two months.
Disease Entity
Frosted Branch Angiitis (FBA) is a rare form of severe retinal vasculitis characterized by diffuse translucent perivascular sheathing of retinal vessels, producing an appearance similar to frost-covered tree branches.
The condition may affect both arteries and veins and is typically associated with extensive retinal inflammation.
FBA was first described in 1976 and may occur as either:
-
Idiopathic frosted branch angiitis usually affects children or young adults with otherwise normal systemic health.
-
Secondary frosted branch angiitis is associated with systemic diseases, infections, or malignancies.
Common secondary causes include viral infections (particularly cytomegalovirus), autoimmune diseases such as systemic lupus erythematosus, and hematologic malignancies such as leukemia or lymphoma.
The condition is notable for its dramatic fundus appearance but often responds well to treatment when appropriately managed.
Pathophysiology
The underlying mechanism of frosted branch angiitis involves severe inflammatory infiltration around retinal vessels, resulting in perivascular edema and accumulation of inflammatory cells.
Histopathologic findings demonstrate:
-
Dense lymphocytic infiltration around retinal vessels
-
Perivascular exudation
-
Endothelial cell injury
The inflammation primarily affects the retinal vasculature rather than the vessel lumen itself. This distinction explains why many patients maintain relatively preserved retinal perfusion despite severe vessel sheathing.
In idiopathic cases, an immune-mediated mechanism is suspected, possibly triggered by viral infection or immune dysregulation. In secondary cases, direct infectious invasion or immune complex deposition may contribute to vascular inflammation.
The resulting perivascular inflammation produces the characteristic translucent white sheathing that extends along the retinal vessels.
Epidemiology
Frosted branch angiitis is rare, with relatively few cases reported in the literature.
Idiopathic FBA most commonly affects children and young adults, often in the second decade of life. Both sexes are affected, although some series suggest a slight female predominance.
Secondary FBA may occur at any age, depending on the underlying cause. In immunocompromised patients, particularly those with HIV infection, cytomegalovirus retinitis can produce a frosted branch angiitis-like appearance.
There is no well-established racial predilection.
Clinical Features
Patients with frosted branch angiitis typically present with acute bilateral visual symptoms.
Common symptoms include:
-
Blurred vision
-
Floaters
-
Photopsias
-
Decreased visual acuity
Symptoms may develop rapidly over days.
Systemic symptoms such as fever, malaise, or viral prodrome may precede ocular involvement, particularly in idiopathic cases.
Visual acuity varies depending on the severity of macular involvement and retinal edema.
Examination Findings
Anterior segment findings may include:
-
Mild anterior chamber cells
-
Keratic precipitates in some cases
Posterior segment findings are striking and include:
-
Diffuse perivascular sheathing of retinal vessels
-
Involvement of both arteries and veins
-
Retinal hemorrhages
-
Macular edema
-
Optic disc edema
-
Vitritis
The characteristic “frosted branch” appearance results from thick, translucent inflammatory sheathing surrounding the retinal vessels.
Fluorescein Angiography (FA)
Typical findings include:
-
Diffuse vascular leakage
-
Staining of vessel walls
-
Areas of capillary nonperfusion in severe cases
-
Macular leakage
Optical Coherence Tomography (OCT)
-
Macular edema
-
Hyperreflective inner retinal inflammation
-
Possible disruption of retinal layers in severe cases
Optical Coherence Tomography Angiography (OCTA)
-
Capillary dropout in areas of ischemia
-
Reduced vascular density in inflamed regions
Differential Diagnosis
Several conditions can mimic the appearance of frosted branch angiitis and must be considered.
Important differential diagnoses include:
-
Cytomegalovirus retinitis
-
Acute retinal necrosis
-
Eales disease
-
Behçet disease
-
Sarcoid retinal vasculitis
-
Leukemic retinopathy
CMV retinitis may produce similar vascular sheathing but is usually accompanied by necrotizing retinitis in immunocompromised patients.
Behçet disease and sarcoidosis can cause severe retinal vasculitis but typically show additional systemic manifestations.
Leukemic infiltration may produce perivascular infiltration and hemorrhages.
Careful systemic evaluation is necessary to exclude these conditions before diagnosing idiopathic FBA.
Diagnosis
Diagnosis of frosted branch angiitis is primarily clinical, based on the characteristic appearance of diffuse perivascular sheathing.
A comprehensive evaluation is essential to determine whether the condition is idiopathic or secondary.
Recommended investigations may include:
-
Complete blood count
-
Inflammatory markers
-
Infectious serologies (HSV, VZV, CMV, syphilis)
-
Tuberculosis screening
-
Autoimmune testing (ANA, ANCA)
In selected cases, imaging studies such as chest radiography or brain MRI may be performed to evaluate systemic disease.
Fluorescein angiography and OCT are important for assessing disease severity and monitoring treatment response.
Management
Management depends on whether the condition is idiopathic or secondary.
Idiopathic Frosted Branch Angiitis
High-dose systemic corticosteroids are the mainstay of treatment. Patients often respond dramatically, with rapid resolution of vascular inflammation.
Treatment typically includes:
-
Oral or intravenous corticosteroids
-
Gradual taper over several weeks
Secondary Frosted Branch Angiitis
Therapy must target the underlying cause. Examples include:
-
Antiviral therapy for CMV or herpes infections
-
Immunosuppressive therapy for autoimmune disease
-
Chemotherapy for hematologic malignancies
Adjunctive treatments may include:
-
Intravitreal anti-VEGF agents for macular edema
-
Immunomodulatory therapy in refractory cases
Regular monitoring with fundus examination, OCT, and FA is recommended.
Prognosis
The prognosis of idiopathic frosted branch angiitis is generally favorable.
With prompt corticosteroid therapy, most patients experience significant visual recovery and resolution of vascular inflammation within weeks.
However, complications may occur, including:
-
Macular edema
-
Retinal ischemia
-
Neovascularization
-
Epiretinal membrane formation
Secondary forms of the disease have a prognosis dependent on the underlying condition.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Uveitis and Ocular Inflammation. San Francisco, CA: AAO; latest edition.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Kleiner RC. Frosted branch angiitis: clinical syndrome or clinical sign? Retina. 1997;17(5):370–371.
-
Walker S, Iguchi A, Jones NP. Frosted branch angiitis: a review. Eye (Lond). 2004;18(5):527–533.
-
Ito Y, Nakano M, Kyu N, et al. Frosted branch angiitis in a child. Jpn J Ophthalmol. 1976;20:92–98.
-
Cunningham ET Jr, Short GA, Irvine AR, Duker JS. Frosted branch angiitis associated with cytomegalovirus retinitis. Ophthalmology. 1995;102(3):417–423.

{kind=link}