
Case Study
A 32-year-old myopic woman presented with a 10-day history of photopsias and a temporal visual field defect in her right eye.


She described shimmering lights and difficulty detecting objects temporally but denied pain or systemic symptoms. Visual acuity was 20/20 in both eyes.
Anterior segment examination was unremarkable, and there was no relative afferent pupillary defect.
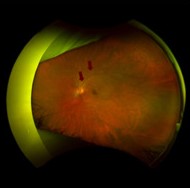
Dilated fundus examination revealed subtle peripapillary outer retinal changes without obvious white dots or hemorrhage.
Optical coherence tomography (OCT) demonstrated focal disruption of the ellipsoid zone in the peripapillary region extending nasally from the fovea.
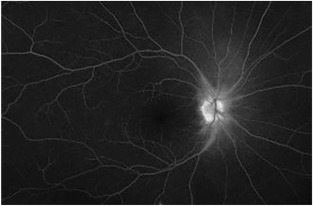
Fundus autofluorescence (FAF) showed a peripapillary hyperautofluorescent ring. Visual field testing revealed a markedly enlarged blind spot in the right eye.
Full-field electroretinography (ERG) was normal, while multifocal ERG showed localized dysfunction corresponding to the affected region.
A diagnosis of Acute Idiopathic Blind Spot Enlargement Syndrome (AIBSES) was made. The patient was observed, and over three months, her photopsias diminished, although the blind spot enlargement partially persisted.
Disease Entity
Acute Idiopathic Blind Spot Enlargement Syndrome (AIBSES) is an uncommon, idiopathic outer retinal disorder characterized by the acute onset of photopsias and enlargement of the physiologic blind spot without significant optic nerve pathology.
It is considered part of the spectrum of white dot syndromes and has overlapping features with Acute Zonal Occult Outer Retinopathy (AZOOR) and Multiple Evanescent White Dot Syndrome (MEWDS).
AIBSES primarily affects the peripapillary outer retina and photoreceptor layer, leading to functional deficits detectable on visual field testing.
Funduscopic findings may be subtle or even normal in early stages, making multimodal imaging crucial for diagnosis.
The condition is typically unilateral and self-limited, though persistent visual field defects are common.
Pathophysiology
The precise pathogenesis of AIBSES remains uncertain. Current evidence supports primary involvement of the outer retina, particularly the photoreceptor outer segments and ellipsoid zone, in the peripapillary region.
OCT studies demonstrate focal disruption of the ellipsoid zone and outer nuclear layer thinning, suggesting photoreceptor dysfunction or loss.
FAF often reveals hyperautofluorescence around the optic disc, indicating metabolic stress at the level of the retinal pigment epithelium (RPE).
Although earlier theories suggested optic nerve involvement, normal visual acuity, absence of afferent pupillary defect, and preserved optic disc structure argue against primary optic neuropathy.
Instead, the blind spot enlargement appears secondary to peripapillary outer retinal dysfunction.
An inflammatory or post-viral immune-mediated mechanism has been proposed, given similarities to other white dot syndromes and occasional viral prodrome.
However, no specific infectious agent or autoimmune marker has been consistently identified.
AIBSES may represent a localized variant within the AZOOR complex, reflecting shared outer retinal pathology.
Epidemiology
AIBSES predominantly affects young to middle-aged adults, with a female predominance. Many patients are myopic.
The condition is rare, and precise incidence data are unavailable. Most reported cases are unilateral, although bilateral involvement has been described rarely.
There is no established racial predilection. Unlike some other inflammatory chorioretinal disorders, AIBSES has no strong association with systemic autoimmune disease.
Clinical Features
Patients with AIBSES typically present with an acute onset of photopsias and visual field abnormalities.
Common symptoms include:
-
Photopsias
-
Subjective scotoma adjacent to fixation
-
Difficulty detecting objects temporally
-
Enlarged blind spot
Visual acuity is usually preserved (20/20 or near normal), which may delay presentation or obscure the severity of the functional deficit.
Pain and systemic symptoms are typically absent. Some patients report a preceding viral-like illness.
The hallmark clinical feature is enlargement of the physiologic blind spot on automated perimetry.
Examination Findings
Anterior segment examination is usually normal.
Funduscopic findings may be subtle and include:
-
Mild peripapillary RPE changes
-
Subtle grayish outer retinal alterations
-
Occasionally minimal vitreous cells
The optic disc generally appears normal, without edema or pallor.
Optical Coherence Tomography (OCT)
-
Peripapillary ellipsoid zone disruption
-
Focal outer nuclear layer thinning
-
Hyperreflective outer retinal changes in the acute phase
Fundus Autofluorescence (FAF)
-
Peripapillary hyperautofluorescent ring
-
Patchy hyperautofluorescence corresponding to affected areas
Fluorescein Angiography (FA)
-
Mild peripapillary window defects
-
Minimal leakage, if any
Indocyanine Green Angiography (ICGA)
-
Hypofluorescent spots in the peripapillary region in some cases
Visual Field Testing
-
Markedly enlarged blind spot
-
Possible adjacent paracentral scotomas
Full-field ERG is typically normal, distinguishing AIBSES from more diffuse outer retinal disorders. Multifocal ERG demonstrates localized dysfunction corresponding to the peripapillary region.
Differential Diagnosis
The differential diagnosis includes:
-
Papilledema
-
Optic neuritis
-
Peripapillary chorioretinitis
-
Acute zonal occult outer retinopathy (AZOOR)
-
Multiple evanescent white dot syndrome (MEWDS)
-
Early glaucoma with peripapillary defects
Papilledema must be excluded, particularly when blind spot enlargement is detected. However, AIBSES lacks optic disc edema and systemic signs of raised intracranial pressure.
Optic neuritis typically presents with decreased visual acuity, pain with eye movement, and afferent pupillary defect.
AZOOR may show more widespread outer retinal dysfunction and progressive zonal field loss.
MEWDS presents with characteristic white dots and wreath-like angiographic findings, which are typically absent in AIBSES.
Careful multimodal imaging and electrophysiology are essential to establish the diagnosis.
Diagnosis
AIBSES is a clinical diagnosis supported by imaging and functional testing.
Key diagnostic criteria include:
-
Acute onset of photopsias
-
Enlarged blind spot on perimetry
-
Preserved visual acuity
-
Peripapillary outer retinal changes on OCT/FAF
-
Normal or near-normal full-field ERG
-
Exclusion of optic nerve pathology
Neuroimaging is not routinely required unless optic nerve disease or intracranial pathology is suspected.
Systemic laboratory testing is generally unnecessary in typical cases.
Management
There is no standardized treatment for AIBSES.
Observation is the primary management strategy, as the condition is often self-limited.
Corticosteroids have been used empirically in some cases, but there is insufficient evidence to support routine use. Given the typically benign course, treatment risks must be weighed carefully.
Patients should be monitored with:
-
Serial visual field testing
-
OCT imaging
-
Symptom assessment
Follow-up is important to ensure stability and to exclude progression toward AZOOR spectrum disorders.
Prognosis
The prognosis of AIBSES is generally favorable in terms of central visual acuity, which usually remains preserved.
However, enlargement of the blind spot may persist partially or completely. Some patients experience gradual improvement over months, while others have stable residual field defects.
Recurrence is uncommon but has been reported.
Long-term progression to more extensive outer retinal disease is rare but warrants continued observation.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Uveitis and Ocular Inflammation. San Francisco, CA: AAO; latest edition.
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Volpe NJ, Rizzo JF 3rd, Lessell S. Acute idiopathic blind spot enlargement syndrome: a review of 27 new cases. Arch Ophthalmol. 2001;119(1):59–63.
-
Gass JDM. Acute zonal occult outer retinopathy and related disorders. Trans Am Ophthalmol Soc. 1993;91:608–665.
-
Monson DM, Smith JR. Acute zonal occult outer retinopathy. Surv Ophthalmol. 2011;56(1):23–35.

{kind=link}