
Case Study
A 54-year-old woman presented with a 4-month history of progressive bilateral visual decline, photopsias, and increasing difficulty with night vision.


She described shimmering lights and intermittent scotomas that were not associated with headache or ocular pain.
Her past medical history was notable for a treated breast carcinoma five years earlier, currently in remission. Visual acuity was 20/40 in both eyes. Anterior segment examination was unremarkable.
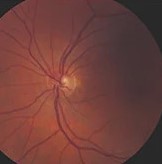
Fundus examination revealed minimal retinal pigment epithelial (RPE) mottling without significant vascular attenuation or optic disc pallor.
Optical coherence tomography (OCT) demonstrated disruption of the ellipsoid zone in the parafoveal region. Full-field electroretinography (ERG) showed markedly reduced photopic and scotopic responses.
Anti-retinal antibody testing revealed circulating antibodies against recoverin and α-enolase. A diagnosis of autoimmune retinopathy (AIR), likely paraneoplastic in origin, was established.
Disease Entity
Autoimmune retinopathy (AIR) is a rare immune-mediated retinal disorder characterized by circulating anti-retinal antibodies leading to progressive photoreceptor dysfunction and vision loss. AIR may be broadly classified into:
-
Paraneoplastic autoimmune retinopathy (pAIR) is associated with systemic malignancy.
-
Cancer-associated retinopathy (CAR)
-
Melanoma-associated retinopathy (MAR)
-
-
Non-paraneoplastic autoimmune retinopathy (npAIR) – occurring in the absence of detectable malignancy.
CAR is most commonly associated with small-cell lung carcinoma, breast carcinoma, and gynecologic malignancies, while MAR is classically linked to cutaneous melanoma.
The disease is characterized by retinal degeneration mediated by autoantibodies directed against retinal antigens such as recoverin, α-enolase, transducin, and others.
AIR is considered a diagnosis of exclusion and requires correlation of clinical findings, electrophysiology, imaging, and serologic testing.
Pathophysiology
The pathogenesis of AIR involves molecular mimicry between tumor antigens (in paraneoplastic forms) or self-antigens (in non-paraneoplastic forms) and retinal proteins.
Tumor cells aberrantly express retinal antigens, triggering an immune response that generates circulating autoantibodies. These antibodies cross the blood-retinal barrier and target photoreceptors and other retinal cells.
Recoverin, a 23-kDa calcium-binding protein involved in phototransduction, is among the best-characterized antigens in CAR. Anti-recoverin antibodies can induce apoptosis in photoreceptors via caspase-dependent pathways.
Similarly, antibodies against α-enolase and other intracellular retinal proteins contribute to retinal degeneration.
Although antibodies are central to the disease mechanism, T-cell–mediated immune responses may also play a role.
The precise mechanism remains incompletely understood, and antibody presence alone does not establish pathogenicity, as low titers may be found in normal individuals or other retinal disorders.
Progressive photoreceptor apoptosis leads to outer retinal atrophy, explaining the discrepancy between early minimal fundus findings and profound electrophysiologic abnormalities.
Epidemiology
AIR is rare, and its true incidence is unknown due to diagnostic challenges and under-recognition. It typically affects middle-aged to older adults but may occur at any age.
Paraneoplastic AIR accounts for a subset of cases and often precedes the diagnosis of systemic malignancy by months.
In CAR, small-cell lung carcinoma is the most frequently associated tumor, followed by breast and gynecologic cancers. MAR is associated with metastatic cutaneous melanoma.
Non-paraneoplastic AIR is more common in women and has been associated with other autoimmune conditions such as systemic lupus erythematosus and autoimmune thyroid disease.
There is no clear racial predilection. Both sexes may be affected, although some series report female predominance in non-paraneoplastic cases.
Clinical Features
Patients with AIR typically present with subacute, progressive, bilateral visual symptoms, although asymmetry may occur.
Common symptoms include:
-
Progressive painless visual loss
-
Photopsias (flashes or shimmering lights)
-
Nyctalopia
-
Photosensitivity
-
Central or paracentral scotomas
-
Peripheral visual field constriction
Symptoms often appear disproportionate to the degree of visible fundus abnormalities. In CAR, vision loss may be rapid and severe.
In MAR, patients often report night blindness and shimmering photopsias, reflecting bipolar cell dysfunction.
Systemic symptoms may relate to underlying malignancy in paraneoplastic cases. Importantly, ocular symptoms may precede cancer diagnosis, necessitating systemic evaluation.
Examination Findings
Anterior segment examination is typically unremarkable.
Fundus findings range from normal in early disease to:
-
Mild RPE mottling
-
Retinal vascular attenuation
-
Optic disc pallor (late)
-
Diffuse retinal atrophy
Optical coherence tomography (OCT) commonly demonstrates:
-
Disruption or loss of the ellipsoid zone
-
Outer nuclear layer thinning
-
Progressive outer retinal atrophy
Fundus autofluorescence (FAF) may show:
-
Parafoveal hyperautofluorescent rings
-
Patchy hypoautofluorescence in advanced stages
Full-field ERG is a hallmark diagnostic tool and typically reveals:
-
Markedly reduced or extinguished photopic and scotopic responses
-
In MAR, a characteristic electronegative ERG (normal a-wave with reduced b-wave), indicating bipolar cell dysfunction
Visual field testing often shows generalized constriction or central scotomas.
Differential Diagnosis
The differential diagnosis of AIR includes:
-
Retinitis pigmentosa
-
Acute zonal occult outer retinopathy (AZOOR)
-
Toxic retinopathies (e.g., hydroxychloroquine toxicity)
-
Infectious retinitis
-
Inherited retinal dystrophies
-
Paraneoplastic optic neuropathy
Distinguishing AIR from inherited retinal degenerations is particularly important. A rapid course, absence of family history, and presence of anti-retinal antibodies favor AIR. Drug toxicity must be carefully excluded.
Because anti-retinal antibodies may be detected in other retinal disorders, serology alone is insufficient for diagnosis.
Diagnosis
AIR is a clinical diagnosis supported by multimodal testing.
Key diagnostic components include:
-
Progressive visual symptoms with minimal fundus findings
-
Abnormal ERG demonstrating retinal dysfunction
-
Presence of circulating anti-retinal antibodies
-
Exclusion of other retinal degenerations
-
Systemic evaluation for malignancy
Systemic workup may include imaging (CT, PET-CT), age-appropriate cancer screening, and referral to oncology when indicated.
There are no universally accepted diagnostic criteria, and expert consensus emphasizes integration of clinical, electrophysiologic, and laboratory findings.
Management
Management of AIR is challenging, and evidence is largely based on case series.
Immunosuppressive Therapy
First-line treatment typically includes systemic corticosteroids. Additional immunomodulatory therapies may include:
-
Mycophenolate mofetil
-
Azathioprine
-
Cyclosporine
-
Intravenous immunoglobulin (IVIG)
-
Rituximab
-
Plasmapheresis
Early initiation may stabilize or slow progression, although visual recovery is uncommon once photoreceptor loss occurs.
Treatment of Underlying Malignancy
In paraneoplastic AIR, control of the primary tumor is essential but does not reliably reverse retinal damage.
Close collaboration with oncology is mandatory.
Monitoring involves serial visual acuity, visual fields, OCT, and ERG.

Prognosis
The prognosis of AIR is variable but often guarded. Many patients experience progressive visual decline despite treatment.
Early detection and prompt immunosuppression may stabilize the disease in some cases. However, irreversible photoreceptor loss frequently results in permanent visual impairment.
Paraneoplastic forms may stabilize with tumor control, but recurrence is possible.
Long-term follow-up is necessary due to potential delayed malignancy detection in initially non-paraneoplastic cases.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Shields CL, Shields JA. Intraocular Tumors: An Atlas and Textbook. 3rd ed. Wolters Kluwer; 2016.
-
Duane TD, Tasman W, Jaeger EA. Duane’s Ophthalmology. Lippincott Williams & Wilkins; latest edition.
-
Heckenlively JR, Ferreyra HA. Autoimmune retinopathy: a review and summary. Semin Immunopathol. 2008;30(2):127–134.
-
Grewal DS, Fishman GA, Jampol LM. Autoimmune retinopathy and antiretinal antibodies: a review. Retina. 2014;34(5):827–845.
-
Adamus G. Autoantibody targets and their cancer relationship in the pathogenicity of paraneoplastic retinopathy. Autoimmun Rev. 2009;8(5):410–414.

{kind=link}