
Case Study
A 29-year-old otherwise healthy woman presented with an acute onset of blurred vision and photopsias in her right eye for one week. She reported a preceding flu-like illness two weeks earlier.

There was no history of autoimmune disease or systemic medication use. Best-corrected visual acuity was 20/60 in the right eye and 20/20 in the left.
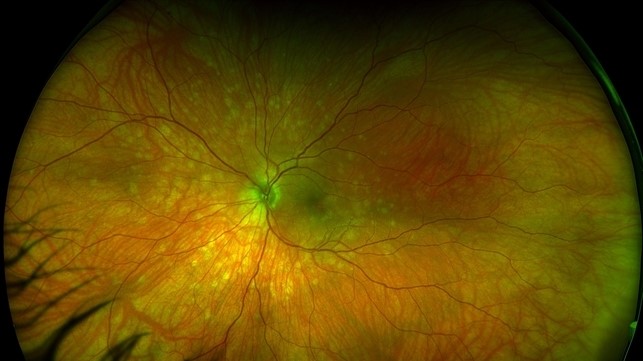
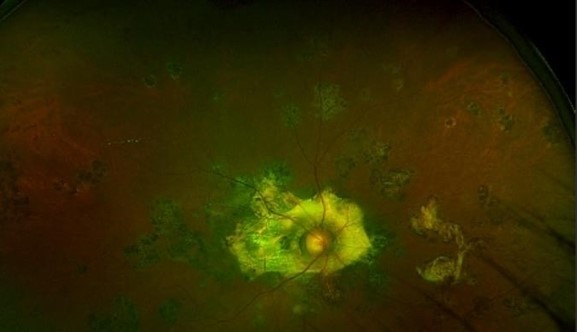
Fundus examination of the right eye revealed multiple small, gray-white dots at the level of the deep retina and retinal pigment epithelium (RPE) in the posterior pole and midperiphery, along with mild foveal granularity. The left eye was normal.
Optical coherence tomography (OCT) demonstrated disruption of the ellipsoid zone and hyperreflective lesions at the outer retina.
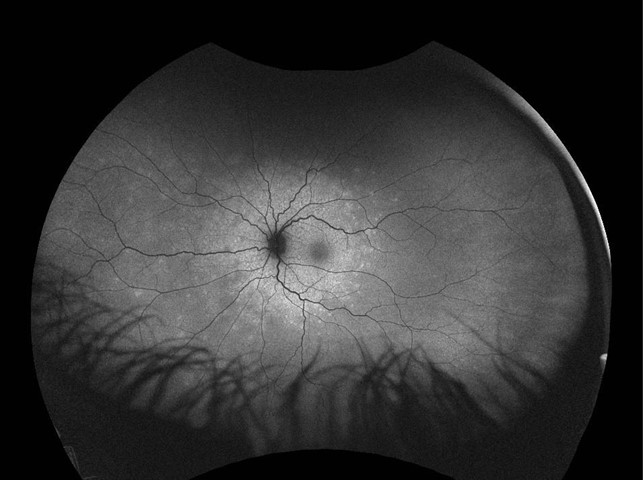
Fundus autofluorescence (FAF) showed multiple hyperautofluorescent spots corresponding to the white lesions.
Fluorescein angiography (FA) revealed early punctate hyperfluorescence in a wreath-like pattern with late staining.
Indocyanine green angiography (ICGA) showed more numerous hypofluorescent lesions than were visible clinically. Full-field electroretinography (ERG) demonstrated a mild transient reduction in photopic responses.
A diagnosis of Multiple Evanescent White Dot Syndrome (MEWDS) was made. The patient was observed without treatment. Visual acuity improved to 20/25 within six weeks, and the white dots resolved spontaneously.
Disease Entity
Multiple Evanescent White Dot Syndrome (MEWDS) is an acute, unilateral, self-limited inflammatory disorder affecting the outer retina, retinal pigment epithelium, and possibly the choriocapillaris.
It belongs to the group of white dot syndromes, a spectrum of inflammatory chorioretinal conditions that share overlapping clinical features.
MEWDS was first described in 1984 and is characterized by multiple small white dots at the posterior pole, foveal granularity, and transient visual dysfunction. The condition is typically unilateral and occurs predominantly in young myopic women.
MEWDS is considered idiopathic, although a viral prodrome and immune-mediated mechanisms are frequently implicated.
Pathophysiology
The precise pathogenesis of MEWDS remains incompletely understood. Current evidence suggests a primary inflammatory process affecting the outer retina, particularly the photoreceptor outer segments and ellipsoid zone.
Earlier theories proposed primary involvement of the choriocapillaris. However, multimodal imaging—particularly spectral-domain OCT and ICGA—supports that the primary site of pathology is the photoreceptor layer with secondary involvement of the RPE and choriocapillaris.
The frequent association with a viral-like prodrome suggests a post-infectious immune-mediated mechanism. Molecular mimicry and transient autoimmune activation may play a role. The self-limited nature of the disease supports a reversible inflammatory or immune dysregulation process rather than structural destruction.
Disruption of the ellipsoid zone on OCT correlates with visual dysfunction, while restoration of outer retinal integrity parallels visual recovery.
Epidemiology
MEWDS predominantly affects young adults, with a strong female preponderance (approximately 70–80%). The typical age range is 20–40 years.
Most cases are unilateral at presentation, although rare bilateral or sequential cases have been reported. Myopia is commonly associated.
A preceding viral-like illness is reported in up to 50% of cases. There is no clear racial predilection. The condition is rare, and the true incidence is unknown due to its self-limited course and possible underdiagnosis.
Unlike some other white dot syndromes, MEWDS has no established association with systemic autoimmune diseases.
Clinical Features
MEWDS typically presents with acute, unilateral visual disturbances.
Common symptoms include:
-
Sudden decrease in visual acuity
-
Photopsias
-
Enlarged blind spot
-
Paracentral scotomas
-
Dyschromatopsia
Symptoms usually develop over days and may follow a viral prodrome. Pain is absent.
Visual acuity at presentation ranges from mild reduction to moderate impairment (commonly 20/40–20/200). The fellow eye is usually asymptomatic and clinically normal.
The hallmark clinical sign is multiple small (100–200 µm), gray-white dots at the posterior pole and midperiphery, often more prominent in the perimacular region.
Foveal granularity is a characteristic finding and may persist even after resolution of white dots.
Examination Findings
Anterior segment examination is typically quiet, although mild vitreous cells may be present.
Fundoscopic findings include:
-
Multiple small white dots at the level of the outer retina/RPE
-
Foveal granularity
-
Mild optic disc edema (occasionally)
Optical Coherence Tomography (OCT)
-
Disruption of the ellipsoid zone
-
Hyperreflective lesions at the outer retina
-
Transient outer nuclear layer changes
Fundus Autofluorescence (FAF)
-
Multiple hyperautofluorescent lesions corresponding to white dots
-
Foveal hyperautofluorescence
Fluorescein Angiography (FA)
-
Early punctate hyperfluorescent spots in a wreath-like pattern
-
Late staining without significant leakage
Indocyanine Green Angiography (ICGA)
-
Numerous hypofluorescent lesions, often more extensive than clinically visible
Visual Field Testing
-
Enlarged blind spot
-
Paracentral scotomas
Full-field ERG may show transient generalized dysfunction, while multifocal ERG demonstrates localized outer retinal impairment.
Differential Diagnosis
MEWDS must be differentiated from other white dot syndromes and inflammatory chorioretinal disorders, including:
-
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
-
Acute zonal occult outer retinopathy (AZOOR)
-
Punctate inner choroidopathy (PIC)
-
Multifocal choroiditis
-
Birdshot chorioretinopathy
-
Viral retinitis
APMPPE typically presents with larger placoid lesions and bilateral involvement.
PIC often affects myopic women but shows punched-out lesions and may lead to choroidal neovascularization (CNV).
AZOOR presents with photopsias and minimal fundus findings but lacks the characteristic white dots of MEWDS. Careful multimodal imaging is essential for accurate differentiation.
Diagnosis
MEWDS is primarily a clinical diagnosis supported by characteristic imaging findings.
Key diagnostic features include:
-
Acute unilateral visual symptoms
-
Multiple small white dots at the posterior pole
-
Foveal granularity
-
Wreath-like hyperfluorescence on FA
-
Ellipsoid zone disruption on OCT
-
Self-limited course
Laboratory investigations are typically unnecessary unless atypical features are present.
Systemic evaluation is not routinely required in typical cases.
Management
MEWDS is generally self-limited and does not require treatment.
Observation is the standard approach in uncomplicated cases. Visual recovery typically occurs within 4–10 weeks.
Corticosteroids are not routinely indicated but may be considered in atypical or severe cases, although evidence supporting their benefit is limited.
Patients should be monitored with serial visual acuity, OCT, and visual field testing until resolution.
Rare complications include persistent blind spot enlargement or, infrequently, secondary choroidal neovascularization.
Prognosis
The prognosis of MEWDS is excellent.
Most patients experience spontaneous recovery of visual acuity within weeks. Structural restoration of the ellipsoid zone on OCT parallels visual improvement.
Mild residual foveal granularity may persist. Recurrences are uncommon but have been reported.
Permanent visual loss is rare, although subtle visual field defects may persist in some cases.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Uveitis and Ocular Inflammation. San Francisco, CA: AAO; latest edition.
-
American Academy of Ophthalmology. Basic and Clinical Science Course (BCSC): Retina and Vitreous. San Francisco, CA: AAO; latest edition.
-
Yanoff M, Duker JS. Ophthalmology. 5th ed. Elsevier; 2019.
-
Jampol LM, Sieving PA, Pugh D, Fishman GA, Gilbert H. Multiple evanescent white dot syndrome. Arch Ophthalmol. 1984;102(5):671–674.
-
Spaide RF, Yannuzzi LA, Slakter JS, Sorenson JA, Orlach DA. Indocyanine green videoangiography of multiple evanescent white dot syndrome. Ophthalmology. 1994;101(5):844–849.
-
Abu-Yaghi NE, Hartono SP, Hodge DO, Pulido JS, Bakri SJ. White dot syndromes: a 20-year study of incidence and outcomes. Ophthalmology. 2011;118(5):1014–1022.

{kind=link}