
Case Study
A 63-year-old male presented with complaints of gradual central vision distortion and blurred vision in his left eye over the past four months.


He denied any history of systemic diseases or previous ocular trauma. His best-corrected visual acuity was 20/30 in the affected eye.
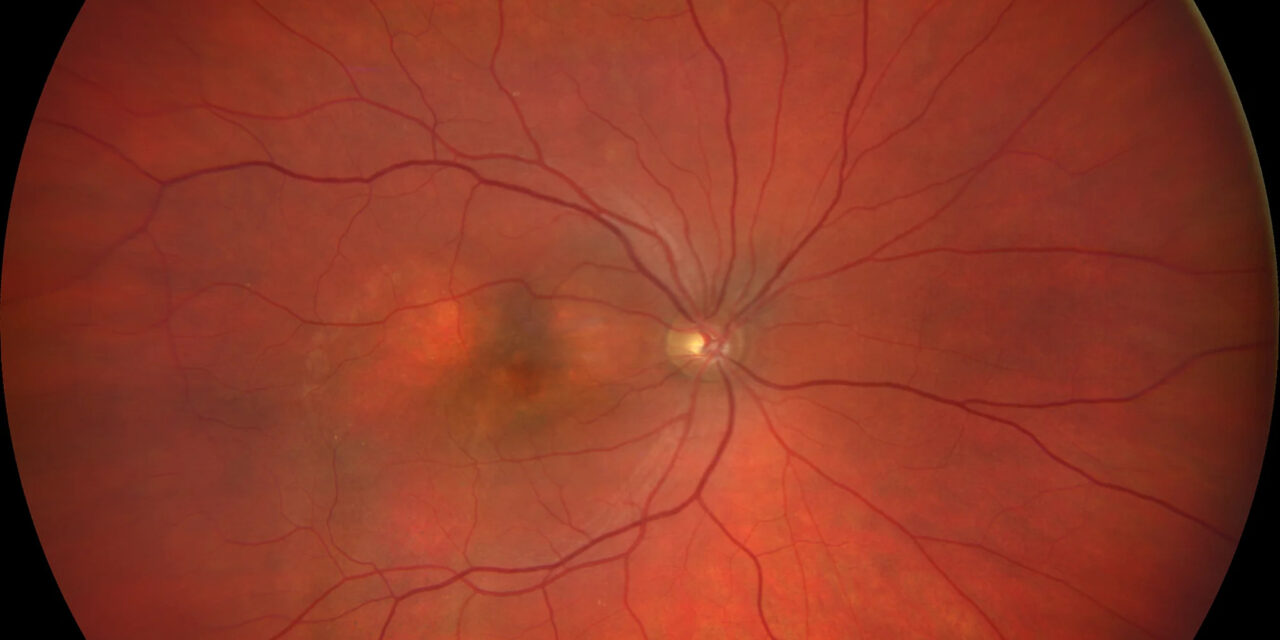
Fundus examination revealed pigmentary changes at the macula with subretinal fluid. Optical coherence tomography (OCT) showed pachychoroid features, including increased choroidal thickness and dilated Haller’s layer vessels.
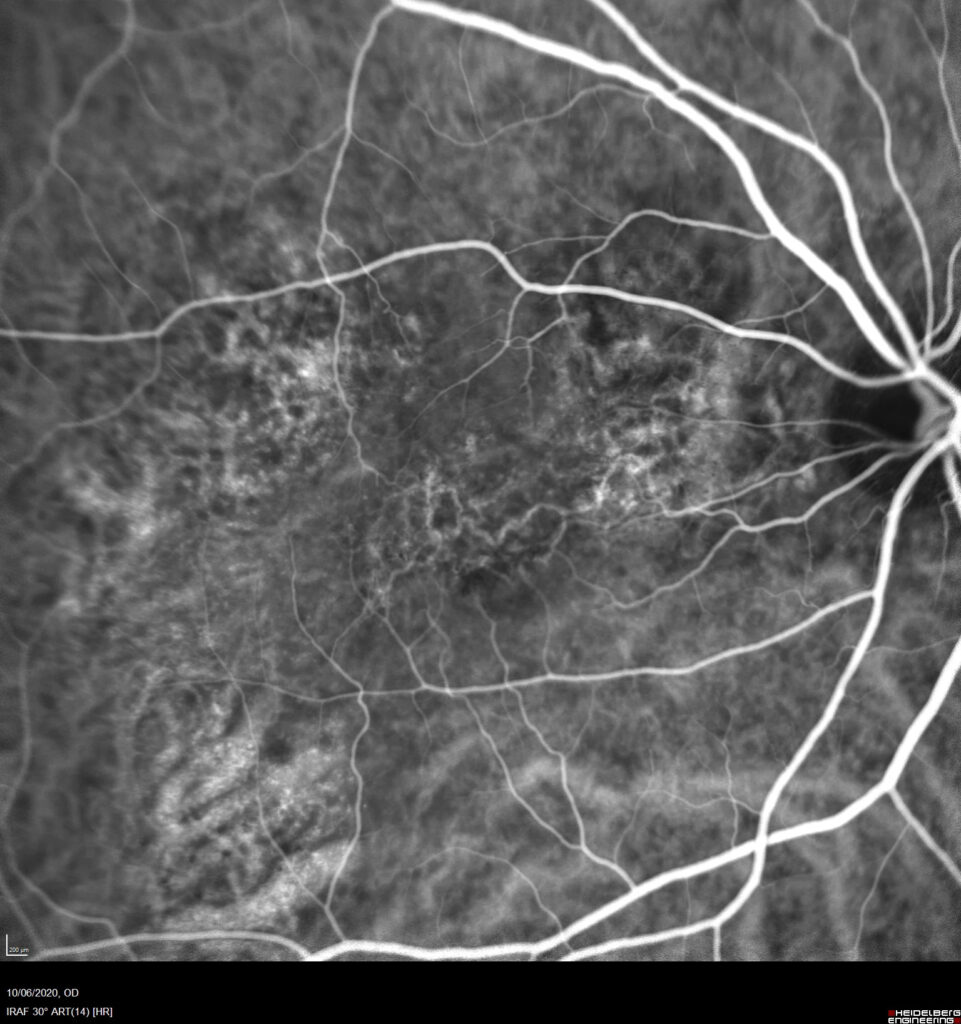
Fundus fluorescein angiography (FFA) and indocyanine green angiography (ICGA) revealed type 1 choroidal neovascularization (CNV).
A diagnosis of Pachychoroid Neovasculopathy (PNV) was made. The patient received intravitreal anti-VEGF therapy with noticeable anatomical and functional improvement.
Disease Entity
Pachychoroid Neovasculopathy (PNV) is a relatively recent and distinct clinical entity within the pachychoroid disease spectrum.
It is characterized by type 1 choroidal neovascularization (CNV) occurring in eyes with a thickened choroid and other features typical of pachychoroidopathies, such as pachyvessels, attenuation of the choriocapillaris, and retinal pigment epithelium (RPE) changes.
Pathophysiology
PNV arises due to chronic choroidal thickening and congestion that leads to RPE stress and subsequent breakdown of Bruch’s membrane.
This chronic stress promotes the development of type 1 CNV beneath the RPE.
The hallmark of pachychoroid spectrum diseases is the presence of dilated outer choroidal vessels (Haller’s layer), which compress the overlying choriocapillaris, potentially leading to hypoxia and neovascularization.
Unlike typical age-related macular degeneration (AMD), drusen are absent or minimal in PNV, suggesting a different pathogenic mechanism.
Epidemiology
PNV is most commonly seen in middle-aged to elderly individuals, often between the ages of 50 and 70.
There is a male predominance, and patients typically present with unilateral symptoms, although bilateral involvement can occur.
It may evolve from other pachychoroid disorders, such as chronic central serous chorioretinopathy (CSCR).
Clinical Features
Patients with PNV often present with:
-
Central vision distortion (metamorphopsia)
-
Blurred vision
-
Relative preservation of visual acuity initially
On fundus examination:
-
Subretinal fluid
-
RPE changes
-
Absence of soft drusen
OCT imaging is critical and typically reveals:
-
Increased subfoveal choroidal thickness (>300 µm)
-
Pachyvessels
-
Type 1 CNV
-
Irregular RPE elevation
-
Subretinal fluid
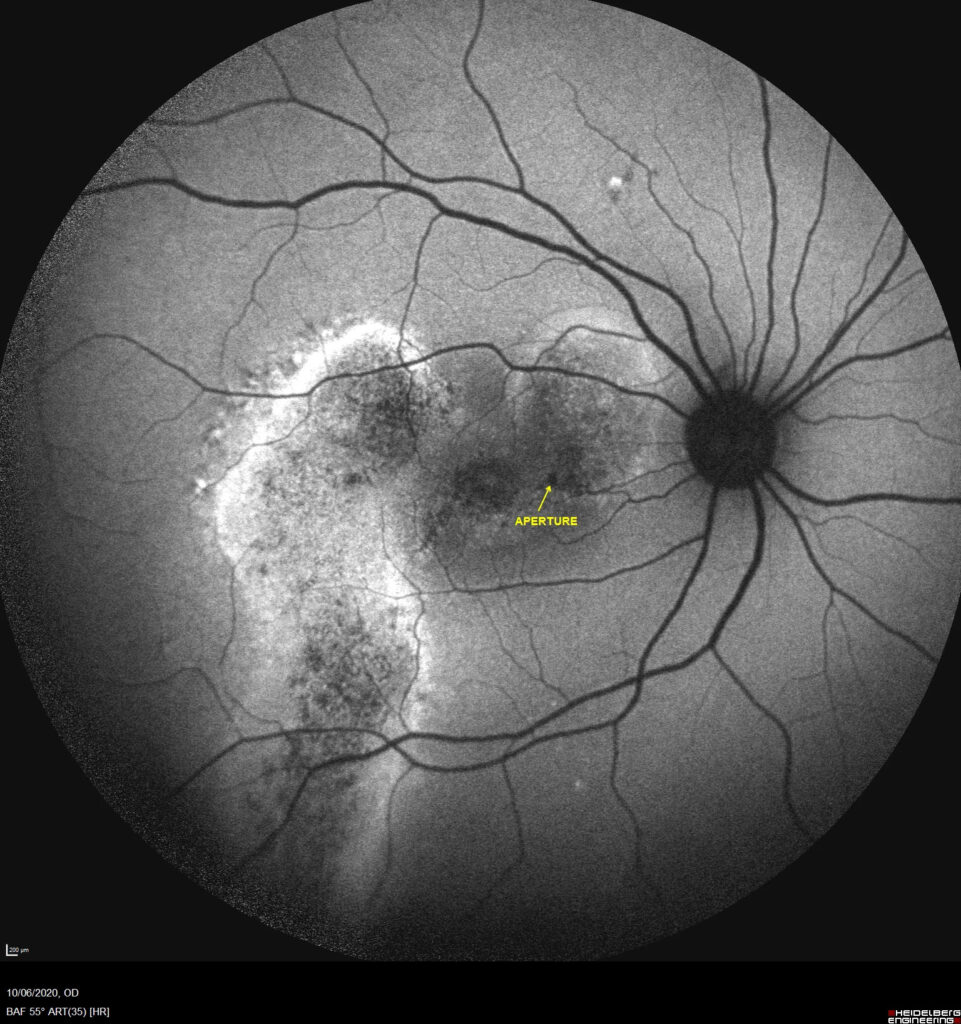
ICGA may show hyperpermeability and dilated choroidal vessels, while FFA reveals leakage from CNV.
Examination Findings
-
Visual Acuity: Mildly to moderately reduced
-
OCT: Subretinal fluid, pachychoroid features, flat, irregular pigment epithelial detachment
-
FFA: Late leakage suggestive of CNV
-
ICGA: Dilated choroidal vessels with hyperpermeability
-
OCT-A: Demonstrates the neovascular network in the avascular outer retina
Differential Diagnosis
-
Neovascular (wet) AMD
-
Polypoidal choroidal vasculopathy (PCV)
-
Chronic central serous chorioretinopathy (CSCR)
-
Idiopathic CNV
-
Pattern dystrophies
Distinguishing features include the absence of drusen and the presence of pachychoroid features without the polyps seen in PCV.
Diagnosis
The diagnosis is based on multimodal imaging findings that include:
-
Type 1 CNV
-
Pachychoroid features on OCT (increased choroidal thickness, pachyvessels)
-
No or minimal drusen
-
ICGA showing choroidal hyperpermeability
OCT-Angiography is particularly helpful in delineating the CNV complex.
Management
Intravitreal Anti-VEGF Therapy:
-
First-line treatment (e.g., ranibizumab, aflibercept, bevacizumab)
-
Typically results in anatomical and visual improvement
Photodynamic Therapy (PDT):
-
Considered in chronic or recurrent cases or when anti-VEGF monotherapy is insufficient
-
Can be used in combination with anti-VEGF for a synergistic effect
Monitoring:
-
Regular follow-up with OCT to monitor CNV activity
-
Adjust treatment interval based on response (treat and extend approach)
Prognosis
With early and appropriate treatment, the prognosis of PNV is generally favorable. Many patients respond well to anti-VEGF therapy, with a reduction in subretinal fluid and stabilization or improvement in visual acuity.
However, recurrence is possible, and some patients may develop chronic disease with RPE damage and fibrosis.
Prevention
As PNV is not associated with traditional AMD risk factors like smoking or drusen, there are no established preventive measures. However:
-
Regular follow-up for patients with pachychoroid features
-
Prompt treatment of CSCR
-
Avoidance of corticosteroid use when not necessary (due to CSCR risk)
References
-
Pang CE, Freund KB. Pachychoroid neovasculopathy. Retina. 2015 Jan;35(1):1-9.
-
Dansingani KK, Balaratnasingam C, Freund KB. Understanding aneurysmal type 1 neovascularization (polypoidal choroidal vasculopathy): A lesson in the taxonomy of “expanded spectra” – A review. Clin Exp Ophthalmol. 2018;46(2):189–200.
-
Miyake M, Ooto S, Yamashiro K, et al. Pachychoroid neovasculopathy and age-related macular degeneration. Sci Rep. 2015;5:16204.
-
Cheung CMG, Lee WK, Koizumi H, Dansingani K, Lai TYY, Freund KB. Pachychoroid disease. Eye. 2019;33(1):14–33.
-
Matsumoto H, Hiroe T, Imai H, et al. Clinical characteristics of pachychoroid neovasculopathy. Invest Ophthalmol Vis Sci. 2015;56(9):620–627.

{kind=link}