
Case Study
A 3-month-old infant was brought to the ophthalmology clinic for poor visual tracking and unusual eye movements.


The child was born with microcephaly to a mother who had experienced a febrile illness with a rash during the first trimester of pregnancy while living in a Zika-endemic region.
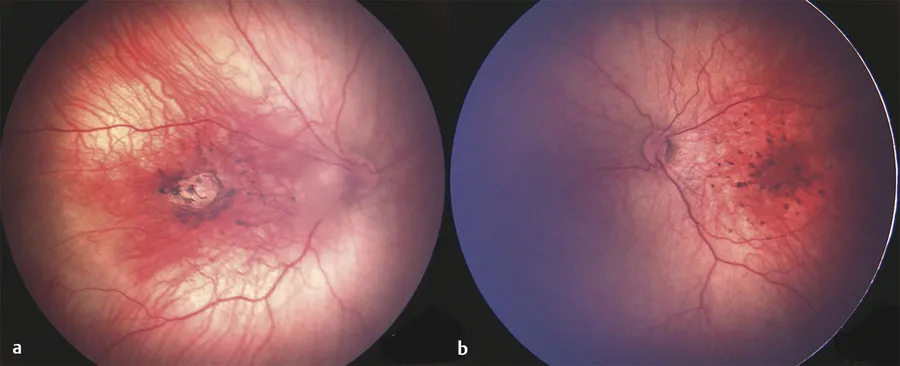
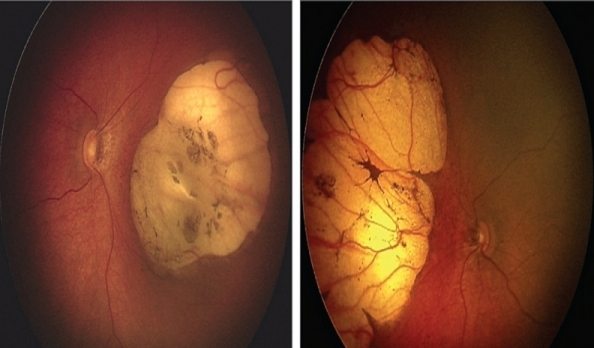
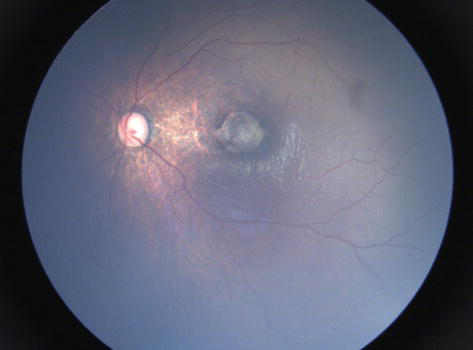
Fundus examination revealed bilateral macular atrophy, pigment mottling, and chorioretinal scarring. Optical coherence tomography (OCT) demonstrated retinal thinning and disruption of the outer retinal layers.
Serological testing confirmed congenital Zika virus infection, leading to a diagnosis of Zika virus retinopathy.
Disease Entity
Zika virus retinopathy is a congenital or acquired retinal disease associated with Zika virus infection, a flavivirus transmitted primarily by Aedes mosquitoes.
While it can cause mild febrile illness in adults, its severe teratogenic effects in fetuses include microcephaly, cerebral calcifications, and retinal damage.
Pathophysiology
Zika virus primarily affects neural progenitor cells, leading to central nervous system and ocular malformations.
Retinal changes result from direct viral invasion, immune-mediated damage, and vascular compromise, leading to:
- Chorioretinal atrophy due to neural tissue destruction.
- Pigmentary changes and mottling from RPE involvement.
- Macular hypoplasia and thinning affect visual function.
Epidemiology
- Transmission: Primarily via Aedes aegypti and Aedes albopictus mosquitoes; also transmitted through vertical (maternal-fetal), sexual, and blood transfusion routes.
- Congenital Zika syndrome (CZS): The most severe manifestations occur with in-utero infection, particularly in the first trimester.
- Outbreaks: Primarily reported in South America, Central America, the Caribbean, and Southeast Asia.
Clinical Features
Congenital Zika Virus Retinopathy
- Microcephaly and neurodevelopmental delay.
- Ocular findings (often bilateral):
- Macular atrophy (foveal or parafoveal).
- Chorioretinal scars (often inferotemporal).
- Retinal vascular abnormalities (attenuated vessels, tortuosity).
- Pigmentary changes resembling congenital toxoplasmosis.
- Optic nerve hypoplasia in some cases.
Acquired Zika Virus Retinopathy (in adults and older children)
- Mild febrile illness with rash, arthralgia, and conjunctivitis.
- Visual disturbances: Blurred vision, photophobia, scotomas.
- Ophthalmic findings:
- Punctate chorioretinal lesions.
- Macular edema and outer retinal disruption.
- Uveitis and vitritis (rare cases).
Examination Findings
- Fundoscopy:
- Macular hypoplasia or atrophy.
- Well-demarcated chorioretinal scars (often inferotemporal).
- Pigmentary changes mimicking other congenital infections.
- Vascular attenuation.
- Optical Coherence Tomography (OCT):
- Outer retinal atrophy in affected areas.
- Thinning of the macula and foveal hypoplasia.
- Fluorescein Angiography (FA):
- Areas of chorioretinal atrophy with reduced perfusion.
- Electroretinography (ERG):
- Reduced scotopic and photopic responses in severe cases.
Differential Diagnosis
- Congenital toxoplasmosis (presents with similar chorioretinal scars but may have active inflammation).
- Congenital cytomegalovirus (CMV) retinopathy (often shows periventricular calcifications and optic atrophy).
- Retinopathy of prematurity (distinguished by a history of premature birth and retinal vascular findings).
- Leber congenital amaurosis (LCA) (typically shows early severe visual impairment and electronegative ERG).
Diagnosis
- Maternal history: Travel or residence in a Zika-endemic region during pregnancy.
- Infant serology and PCR:
- Zika virus IgM/IgG antibodies.
- Reverse transcription polymerase chain reaction (RT-PCR) in serum, urine, or cerebrospinal fluid (CSF).
- Neuroimaging (MRI or CT):
- Intracranial calcifications, ventriculomegaly, corpus callosum abnormalities.
- Ophthalmic imaging:
- OCT, FA, and ERG for retinal assessment.
Management
There is no specific antiviral therapy for Zika virus. Management focuses on supportive care and early intervention.
Neonatal and Pediatric Management
- Multidisciplinary care (neurology, ophthalmology, developmental specialists).
- Low vision rehabilitation if visual impairment is significant.
- Early intervention programs (occupational and visual therapy).
Adult Management
- Self-limiting in most cases.
- Ocular complications (macular edema, uveitis) may require corticosteroids.
Prognosis
- Congenital Zika virus retinopathy: Permanent vision loss is common due to macular atrophy and optic nerve involvement.
- Acquired Zika virus retinopathy: Generally mild and self-limiting, with good visual recovery in most cases.
Conclusion
Zika virus retinopathy is a significant infectious retinal disorder, particularly in congenital cases, where it leads to chorioretinal atrophy, macular hypoplasia, and vascular changes.
Early detection and multidisciplinary care are essential for optimizing outcomes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Ventura CV, Maia M, Bravo-Filho V, et al. “Zika virus in Brazil and macular atrophy in a child with microcephaly.” Lancet. 2016;387(10015):228.
- de Paula Freitas B, de Oliveira Dias JR, Prazeres J, et al. “Ocular findings in infants with microcephaly associated with presumed Zika virus congenital infection in Salvador, Brazil.” JAMA Ophthalmol. 2016;134(5):529-535.
- Yepez JB, Murati FA, Pettito M, et al. “Ocular manifestations of Zika virus infection in adults.” JAMA Ophthalmol. 2017;135(5):538-545.
- Torres Netto EA, Al-Dahmash SA, Salomão DR, et al. “Ophthalmic manifestations of congenital Zika syndrome: A systematic review.” J Pediatr Ophthalmol Strabismus. 2020;57(2):89-98.

{kind=link}