
Case Study
A 57-year-old woman presented with a gradual loss of vision in her left eye and mild discomfort over three months. Her medical history included poorly controlled hypertension and primary open-angle glaucoma.

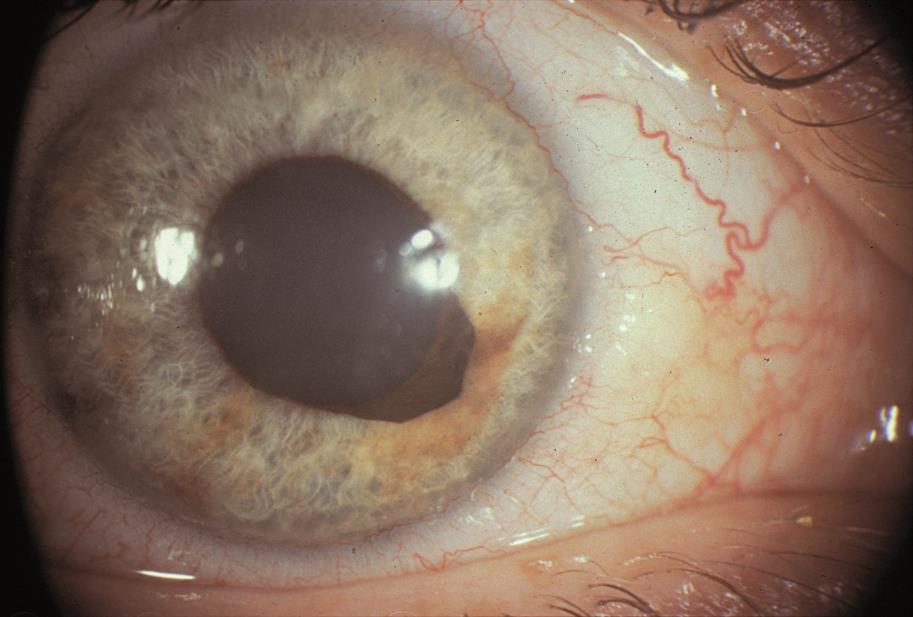
On slit-lamp examination, her left iris showed an outward curling of the pigmented epithelium at the pupillary margin, characteristic of ectropion uveae.
Gonioscopy revealed angle narrowing, and intraocular pressure (IOP) was elevated at 28 mmHg in the affected eye.
Fundoscopy demonstrated advanced optic nerve cupping with no signs of diabetic retinopathy or retinal vein occlusion.
Following a detailed workup, including imaging to rule out neoplasms, she was diagnosed with acquired ectropion uveae secondary to glaucoma.
She underwent IOP-lowering treatment, but her visual prognosis remained guarded due to advanced optic nerve damage.
Disease entity
Acquired ectropion uvea (AEU) is a rare but clinically significant condition characterized by an outward turning of the pigmented iris epithelium at the pupillary margin.
Unlike congenital ectropion uveae, AEU is not developmental but results from underlying ocular or systemic conditions.
It is frequently associated with conditions that cause structural alterations in the iris, such as neovascularization, glaucoma, or intraocular tumors.
Early identification is crucial as AEU often signals serious underlying pathology requiring immediate attention.

Pathophysiology
The pathogenesis of AEU involves structural and functional disruptions of the iris due to various underlying causes:
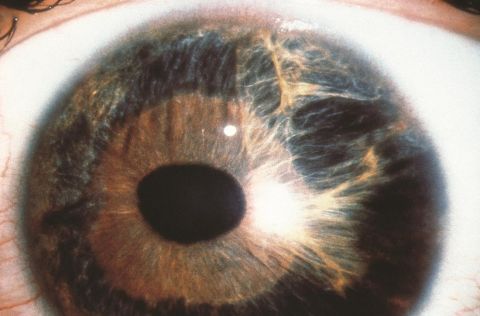
- Iris Neovascularization:
- The proliferation of abnormal blood vessels on the iris surface induces tractional forces, leading to the outward curling of the pigmented epithelium.
- Glaucoma and Elevated IOP:
- Chronic elevated IOP may deform the iris architecture, resulting in ectropion uveae.
- Inflammatory and Tumor-Associated Changes:
- Inflammatory conditions or intraocular tumors can cause local traction or infiltration of the iris, contributing to ectropion.
Epidemiology
- Incidence and Prevalence:
- AEU is rare, with its exact prevalence unknown.
- Age and Gender Predilection:
- Typically seen in adults, with no strong gender predilection.
- Risk Factors:
- Ocular conditions such as glaucoma, iris neovascularization, or trauma.
- Systemic conditions like diabetes mellitus or neoplastic syndromes.
Clinical Features
Patients with AEU may present with various symptoms and signs depending on the underlying cause:
- Symptoms:
- Gradual or acute vision loss.
- Photophobia and glare.
- Redness or discomfort if associated with inflammation.
- Signs:
- Slit-Lamp Examination:
- Outward curling of the pigmented iris epithelium at the pupillary margin.
- Associated findings: iris neovascularization, synechiae, or irregular pupils.
- IOP Assessment:
- Often elevated in glaucoma-associated AEU.
- Slit-Lamp Examination:
Examination Findings
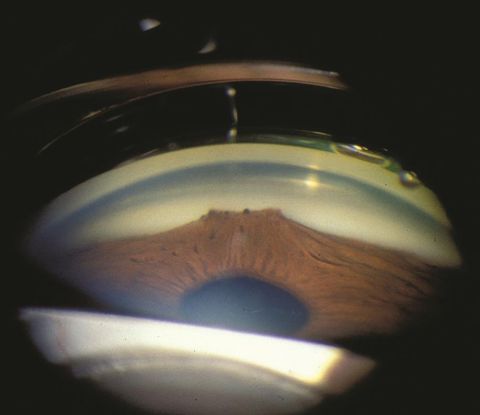
- Gonioscopy:
- Iridocorneal angle narrowing or closure.
- Presence of abnormal blood vessels in cases of neovascularization.
- Fundoscopy:
- Optic nerve damage in glaucoma-associated cases.
- Anterior Segment Imaging:
- Ultrasound biomicroscopy (UBM) or anterior OCT may reveal structural iris changes.
Differential Diagnosis
- Congenital ectropion uveae.
- Neovascular glaucoma.
- Iris rubeosis.
- Intraocular tumors (e.g., melanoma).
- Chronic iridocyclitis.
Diagnosis
The diagnosis of AEU relies on clinical examination and imaging to determine the underlying cause:
- Slit-Lamp Examination: Identification of ectropion at the pupillary margin.
- Imaging: Anterior OCT or UBM to assess iris structure.
- Laboratory Workup: In cases of suspected systemic involvement, tests such as fluorescein angiography may help assess vascular changes.
Management
The treatment of AEU focuses on addressing the underlying cause while managing its ocular complications:
- Underlying Cause Treatment:
- Neovascularization: Panretinal photocoagulation (PRP) or anti-VEGF injections.
- Glaucoma: IOP-lowering medications, laser therapy, or surgical intervention.
- Inflammation: Corticosteroids or immunomodulatory therapy as needed.
- Tumors: Surgical removal or oncologic treatment based on tumor type.
- Symptomatic Management:
- Corrective lenses or assistive devices for visual impairment.
- Patient Monitoring:
- Regular IOP monitoring and optic nerve evaluation.
Prognosis
The prognosis for AEU varies widely depending on the underlying etiology and the timeliness of intervention.
While IOP control can slow glaucomatous damage, irreversible vision loss may occur if the condition is diagnosed late.
Patients with neovascularization or intraocular tumors require close monitoring for recurrence or metastasis.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Shields, M. B., & Shields, J. A. (1998). Acquired ectropion uveae: Classification and clinical implications. Survey of Ophthalmology, 42(1), 71-81.
- Jonas, J. B., & Xu, L. (2014). Glaucoma and iris changes: Insights into ectropion uveae. Acta Ophthalmologica, 92(6), e445-e451.
- Boyce, J. F., & Mendicino, M. E. (2007). Acquired ectropion uveae secondary to rubeosis iridis. Archives of Ophthalmology, 125(5), 720-721.
- Cohen, S. Y., & Massin, P. (2003). Clinical spectrum of acquired ectropion uveae in neovascular glaucoma. British Journal of Ophthalmology, 87(8), 956-961.
- Spaide, R. F. (2012). Advances in anterior segment imaging: Relevance to ectropion uveae. Ophthalmology Clinics of North America, 25(4), 627-641.

{kind=link}