
Case Study
A 24-year-old woman with a ten-year history of poorly controlled Type 1 diabetes mellitus presented with complaints of progressively worsening blurred vision and glare sensitivity over three months.


She reported difficulties in recognizing faces and reading, significantly impacting her daily life. Her blood glucose levels had been erratic, with a recent HbA1c of 12%.
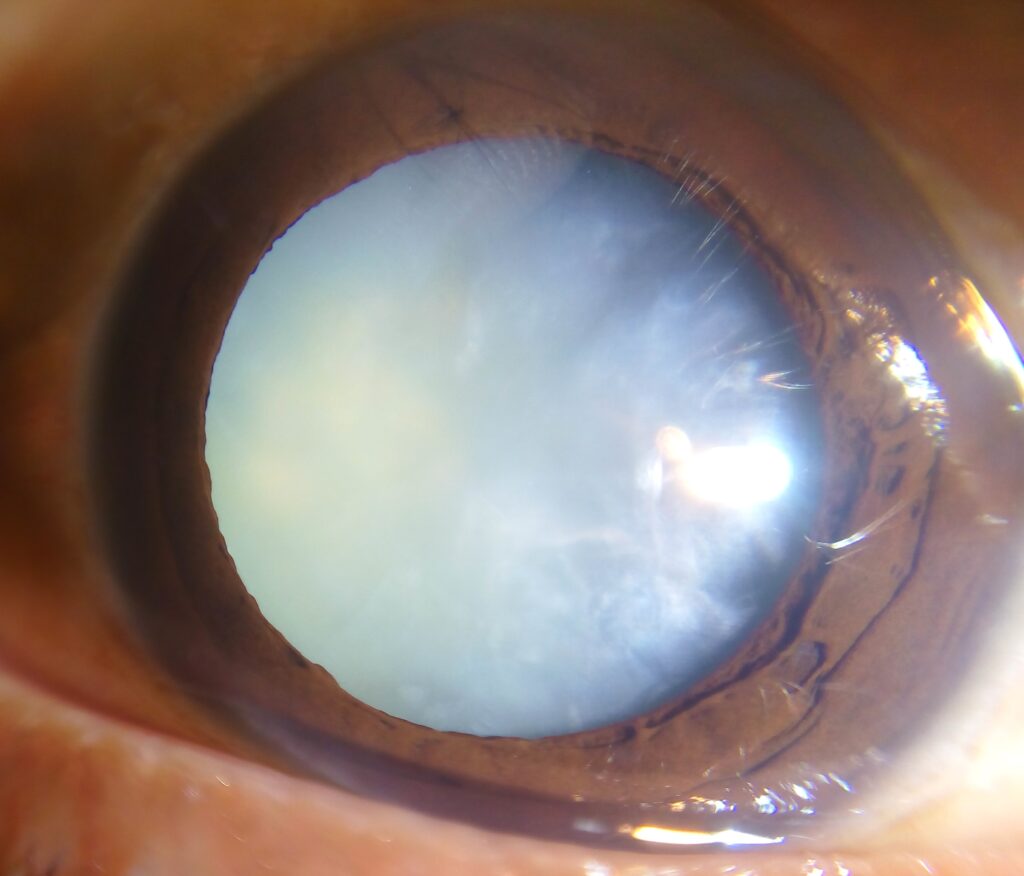
On examination, bilateral snowflake-like opacities were observed in the lens cortex on slit-lamp examination. Fundoscopy revealed no diabetic retinopathy.
Optical coherence tomography (OCT) of the retina was normal. Given the rapid progression of her visual symptoms, cataract surgery with intraocular lens implantation was performed.
Postoperatively, her uncorrected visual acuity improved to 20/20 in both eyes. She was referred to a diabetologist for better glycemic control.
Disease entity
Snowflake cataract is a rare and visually significant lens opacity primarily seen in young individuals with poorly controlled diabetes mellitus.
First described in the 19th century, it is characterized by its distinct snowflake-like appearance within the cortical layers of the lens.
The condition is notable for its rapid progression compared to other forms of cataracts.

Unlike age-related cataracts, snowflake cataracts are closely tied to systemic hyperglycemia, making their management dependent not only on surgical intervention but also on stringent diabetic control.
The condition emphasizes the interplay between systemic metabolic dysfunction and ocular health.
Pathophysiology
The pathogenesis of snowflake cataracts revolves around the biochemical effects of hyperglycemia on the lens:
- Polyol Pathway Activation
- Glucose enters the lens via facilitated diffusion and is converted into sorbitol by aldose reductase.
- Sorbitol, being osmotically active and poorly diffusible, accumulates within the lens, leading to water influx and osmotic stress.
- Oxidative Stress
- Chronic hyperglycemia results in the generation of reactive oxygen species (ROS).
- ROS causes oxidative damage to lens proteins and lipids, leading to structural instability and cataract formation.
- Protein Denaturation and Aggregation
- High glucose concentrations disrupt lens protein folding, resulting in aggregation and opacification.
- Lens Metabolism Disruption
- Hyperglycemia alters the ionic and metabolic balance of lens fibers, exacerbating damage and opacity formation.
Epidemiology
- Incidence and Prevalence:
Snowflake cataracts are rare and primarily seen in young patients with uncontrolled Type 1 or Type 2 diabetes. - Geographic and Ethnic Variability:
The condition is reported globally but may be more frequently observed in regions with limited access to healthcare or insulin therapy. - Risk Factors:
- Poor glycemic control (HbA1c >9%)
- Duration of diabetes, especially in juvenile-onset cases
- Lack of timely diabetes management or education
Clinical Features
Snowflake cataracts present with the following symptoms and signs:
- Symptoms:
- Progressive, bilateral visual impairment
- Increased sensitivity to bright light and glare
- Difficulty with near and distance vision
- Rapid onset of visual symptoms compared to age-related cataracts
- Signs:
- Slit-Lamp Examination:
- Multiple snowflake-shaped opacities scattered in the lens cortex
- White or gray opacities with a crystalline appearance
- Fundoscopy:
- Typically normal unless coexisting diabetic retinopathy is present
- Slit-Lamp Examination:
Examination Findings
- Visual Acuity Testing: Reduced bilateral acuity proportional to the cataract severity
- Slit-lamp Biomicroscopy: Distinctive snowflake-shaped opacities localized in the cortical region of the lens
- Additional Testing:
- Optical Coherence Tomography (OCT) to rule out diabetic macular edema
- Fundus photography to evaluate for diabetic retinopathy
Differential Diagnosis
- Age-related cortical cataracts
- Diabetic myopia (due to lens swelling)
- Posterior subcapsular cataracts (seen in diabetes)
- Christmas tree cataract
- Drug-induced cataracts (e.g., steroids)
Diagnosis
The diagnosis of snowflake cataract is clinical, relying on slit-lamp findings in a patient with poorly controlled diabetes. Supporting diagnostic measures include:
- Blood glucose and HbA1c testing to confirm poor glycemic control
- Exclusion of other causes of cortical lens opacities
Management
Treatment strategies for snowflake cataracts focus on improving vision through surgical and medical interventions:
- Surgical Management:
- Phacoemulsification with intraocular lens implantation is the definitive treatment.
- Early surgical intervention is often necessary due to the rapid progression of lens opacities.
- Diabetes Management:
- Intensive blood glucose control through insulin or oral hypoglycemic agents
- Dietary modifications and lifestyle changes
- Regular endocrinology follow-ups
- Patient Education:
- Emphasis on the importance of diabetes management to prevent recurrence
- Awareness about potential long-term complications such as retinopathy
- Postoperative Care:
- Monitoring for surgical complications such as posterior capsule opacification (PCO)
- Regular screening for diabetic retinopathy
Prognosis
Patients with snowflake cataracts typically experience excellent visual recovery after cataract surgery, provided diabetes is well-managed.
![]()
However, continued poor glycemic control may lead to recurrence or other ocular complications, such as diabetic retinopathy or macular edema.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Kinoshita, J. H. (1990). Mechanisms initiating cataract formation: Proctor Lecture. Investigative Ophthalmology & Visual Science, 31(5), 891-899.
- Brownlee, M. (2001). Biochemistry and molecular cell biology of diabetic complications. Nature, 414(6865), 813-820.
- Jeon, S., Lee, W. K., & Kim, Y. J. (2018). Outcomes of cataract surgery in young diabetic patients with snowflake cataracts. American Journal of Ophthalmology, 186, 97-103.
- Pollreisz, A., & Schmidt-Erfurth, U. (2010). Diabetic cataract—pathogenesis, epidemiology, and treatment. Journal of Ophthalmology, 2010, 608751.
- Jonas, J. B., & Panda-Jonas, S. (2014). Diabetes mellitus and cataract: Progression and management. Ophthalmology Clinics of North America, 27(4), 399-413.
- Spaide, R. F. (2018). Diabetic lens changes and their implications. Retina, 38(4), 708-716.

{kind=link}