
Case Study
A 65-year-old man with a history of cutaneous melanoma presented with complaints of night vision difficulty, shimmering lights, and a sensation of flickering in his peripheral vision.

He had no history of retinal disease, and his melanoma was treated a year prior with no evidence of recurrence.
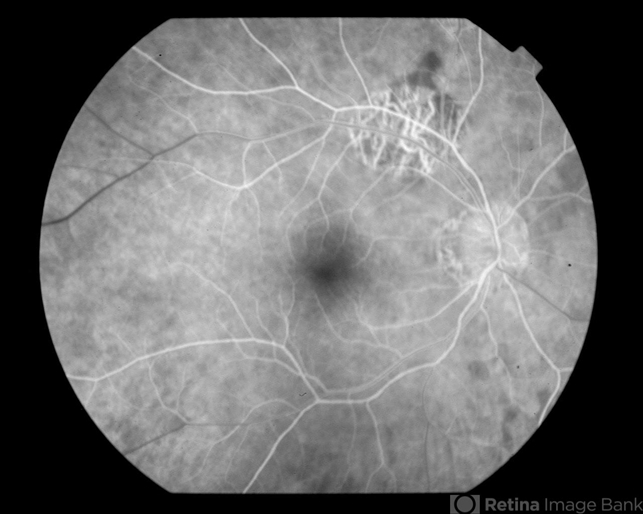
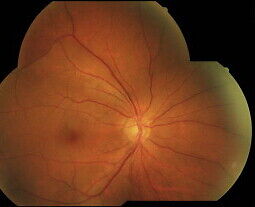
Ophthalmic examination revealed a normal fundus, but electroretinography (ERG) demonstrated abnormalities consistent with an inner retinal dysfunction.
Subsequent serum analysis revealed the presence of autoantibodies against retinal bipolar cells, confirming the diagnosis of Melanoma-associated retinopathy (MAR).
Treatment with immunosuppressive therapy was initiated to mitigate symptoms, and the patient was closely monitored for melanoma recurrence.
Introduction
Melanoma-associated retinopathy (MAR) is a paraneoplastic syndrome in which patients with cutaneous or, less commonly, uveal melanoma develop autoimmunity against retinal cells, specifically the bipolar cells.
The result is a form of non-hereditary, bilateral retinopathy that affects visual function. MAR typically presents with symptoms like photopsias (flashing lights), night vision difficulty, and a shimmering sensation, often preceding or coinciding with melanoma recurrence.
While the exact pathogenesis remains unclear, the condition is hypothesized to involve melanoma-related autoantibodies cross-reacting with retinal antigens, disrupting retinal signal transduction.

Pathophysiology
The pathogenesis of MAR is related to an autoimmune reaction in which antibodies produced against melanoma antigens cross-react with retinal antigens, specifically those found in retinal bipolar cells.
This autoimmune attack leads to retinal dysfunction, especially affecting the ON-bipolar cells and disrupting signal transmission from the photoreceptors to the ganglion cells.
These autoantibodies also impact the electroretinogram (ERG) response, resulting in a characteristic ‘negative ERG’ where the b-wave is significantly reduced, representing inner retinal dysfunction.
Melanoma-associated retinopathy (MAR) is part of a broader group of paraneoplastic retinopathies in which cancers outside the eye cause retinal changes due to immune-mediated mechanisms.
Epidemiology
Melanoma-associated retinopathy (MAR) is rare and primarily affects patients with a history of cutaneous melanoma, usually detected in middle-aged to older adults.
It can occur in both men and women, but its exact prevalence is unknown due to its rarity and the overlap of symptoms with other retinopathies.

Reports have indicated that Melanoma-associated retinopathy (MAR) may appear years after the initial melanoma diagnosis or, in some cases, it may be the presenting symptom of melanoma metastasis, underscoring the importance of comprehensive evaluation in patients with unexplained visual symptoms.
Clinical Features
Patients with MAR often experience:
- Photopsias: Flashing lights or shimmering in the visual field, often worse in low light.
- Nyctalopia: Difficulty with night vision is a common symptom due to impaired function of the retinal bipolar cells.
- Visual Distortions: Flickering or shimmering, especially in peripheral vision, and occasional color vision changes.
- Central Vision: In the early stages, central vision may be preserved, but peripheral vision is often affected.
Examination Findings
- Fundus Exam: Often appears normal or may reveal subtle pigmentary changes, as MAR typically affects inner retinal function rather than causing visible structural changes.
- ERG: The hallmark finding in Melanoma-associated retinopathy (MAR) is a “negative ERG” pattern with a normal a-wave and a severely diminished b-wave, suggesting bipolar cell dysfunction.
- Autoantibody Testing: The presence of anti-retinal antibodies, specifically against ON-bipolar cells, helps confirm the diagnosis in conjunction with clinical findings.
Differential Diagnosis
- Cancer-associated retinopathy (CAR)
- Retinitis pigmentosa
- Autoimmune retinopathy
- Acute zonal occult outer retinopathy (AZOOR)
- Central serous chorioretinopathy (CSCR)
Management
Treatment of Melanoma-associated retinopathy (MAR) primarily involves immunosuppressive therapy to reduce autoimmune activity and alleviate symptoms.
Commonly used agents include corticosteroids, intravenous immunoglobulin (IVIG), and other immunosuppressants like methotrexate.
Plasmapheresis has been utilized in severe cases to remove circulating autoantibodies. Management also includes regular follow-up to monitor for potential melanoma recurrence, as Melanoma-associated retinopathy (MAR) can be a sign of tumor progression.
Prognosis
The prognosis for Melanoma-associated retinopathy (MAR) varies; while immunosuppression can improve symptoms in some patients, others may experience persistent or progressive visual dysfunction.
Additionally, the presence of MAR is associated with a high risk of melanoma recurrence, underscoring the need for vigilant oncologic follow-up.
Early detection and management are critical in preserving visual function and addressing potential melanoma activity.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Alexander, K. R., & Fishman, G. A. (1989). Rod dysfunction in melanoma-associated retinopathy. Archives of Ophthalmology, 107(2), 241-244.
- Berson, E. L., Lessell, S., & Gragoudas, E. S. (1983). Paraneoplastic night blindness with cutaneous malignant melanoma. American Journal of Ophthalmology, 96(2), 267-275.
- Lu, Y., Jia, L., & Crosson, J. N. (2017). Clinical and electrophysiological characterization of melanoma-associated retinopathy. American Journal of Ophthalmology, 183, 83-91.
- Weleber, R. G., & Watzke, R. C. (1981). Electrophysiologic testing in melanoma-associated retinopathy. Archives of Ophthalmology, 99(8), 1282-1284.
- Darnell, R. B., & Posner, J. B. (2003). Paraneoplastic syndromes involving the nervous system. New England Journal of Medicine, 349(16), 1543-1554.

{kind=link}