
CASE REPORT
A 45-year-old man was referred to the ocular oncology service for evaluation due to a black asymptomatic lesion in his right eye. His medical history included hyperlipidemia and high myopia.

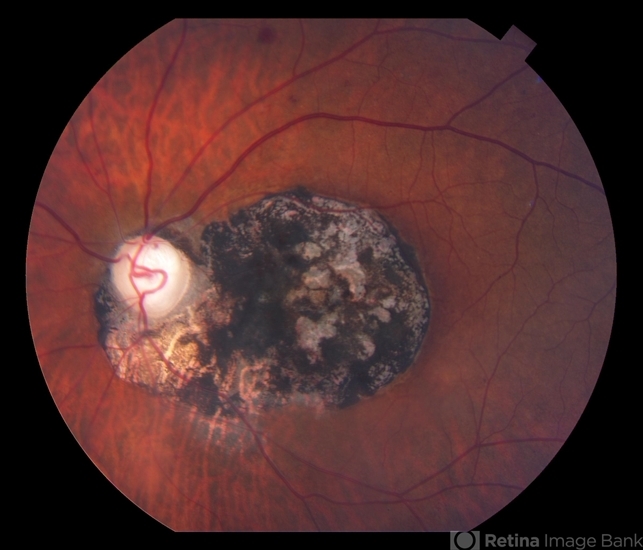
On clinical examination, a flat black lesion that looked like a flower was observed. The lesion did not resemble melanoma. Moreover, an ultrasound examination confirmed that the lesion was flat.
The lesion showed hypo autofluorescence at the dark parts that correlate with the known histopathologic evidence of lack of lipofuscin in the retinal pigment epithelium of congenital hypertrophy of retinal pigment epithelium (CHRPE) and mild hyper autofluorescence that correlate with scleral autofluorescence at the lacunae.
In optical coherence tomography, a loss of the external retinal layers was seen in the area of the lesion and no retina was seen in the lacunae’ area. The diagnosis was confirmed as Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE).
Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE) DISEASE entity
Congenital hypertrophy of the retinal pigment epithelium (CHRPE) is a typically benign, asymptomatic, pigmented fundus lesion. It is a congenital hamartoma of the retinal pigment epithelium (RPE) and occurs in three variant forms: solitary (unifocal), grouped (multifocal), and atypical.

Atypical CHRPE is associated with familial adenomatous polyposis (FAP), an autosomal dominant cancer syndrome, characterized by numerous adenomatous polyps of the colon and rectum. Left untreated, virtually all FAP patients develop colorectal carcinoma/s by middle age.
FAP sub-types, including Gardner syndrome (FAP plus skeletal hamartomas and various soft tissue tumors) and Turcot syndrome (FAP plus various brain tumors), are also associated with atypical CHRPE.
The prevalence of CHRPE in the general optometric population has been estimated to be 1.2%. Atypical CHRPE is the earliest and most common extra-colonic manifestation of FAP, present in up to 90% of patients.
Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE) Diagnosis
The diagnosis of CHRPE is usually made clinically and no diagnostic procedures are generally necessary. Fundus photography is useful for documentation and follow-up of lesions and wide-field scanning-laser ophthalmoscopy has been recommended as a screening tool.

Ancillary testing may be beneficial in uncertain cases.
- Lesions typically demonstrate hypo autofluorescence on fundus autofluorescence (FAF) due to their high melanin content. Non-pigmented haloes or lacunae may show autofluorescence.
- No leakage is demonstrated on fluorescein angiography (FA) or indocyanine green angiography (ICGA). Lesions typically block underlying choroidal fluorescence, except in areas of depigmented lacunae or haloes.
- Optical coherence tomography findings include retinal thinning and photoreceptor loss over lesions, with the absence of RPE and increased transmission of light in areas of lacunae.
- The use of Optical coherence tomography angiography (OCTA) in the evaluation of CHRPE has limitations due to thick RPE and increased cumulative melanin granules. However, this modality is better than FA or ICG in visualizing choroidal vasculature.
- Electroretinogram (ERG), electrooculogram (EOG), A-scan, and B-scan ultrasonography are non-contributory.
Differential diagnosis
- Choroidal melanoma
- Choroidal nevus
- Melanocytoma
- Focal pigmentation (caused by injury, inflammation, or drug toxicity)
- True hyperplasia of the RPE
- Black sunburst lesion in sickle cell retinopathy
- Congenital grouped albinotic retinal pigment epithelial spots (CGARPES) (“polar bear tracks”) may resemble grouped CHRPE but are characterized by multiple grouped, white, variably-sized, albinotic spots of the RPE. The nature of these lesions has not been investigated histologically.
MANAGEMENT of Congenital Hypertrophy of the Retinal Pigment Epithelium (CHRPE)
No active intervention is generally indicated or required. Proton beam therapy has been described for rare complicated cases.

Complications
CHRPE lesions have been documented to enlarge in 46-83% of cases over at least three years of follow-up. The foveal extension may result in impaired visual acuity.
Rarely, nodular pigmented adenocarcinomas may arise from within areas of CHRPE. Untreated nodular lesions have been documented to progress to pedunculated tumors with associated serous retinal detachment.
Premacular gliosis and cystoid macular edema are frequently seen when peripheral pigmented or non-pigmented RPE tumors arise within CHRPE.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Coleman P, Barnard NA. Congenital hypertrophy of the retinal pigment epithelium: prevalence and ocular features in the optometric population. Ophthalmic Physiol Opt. 2007;27:547–555.
- Wallis YL, Macdonald F, Hulten M, et al: Genotype-phenotype correlation between position of constitutional APC gene mutation and CHRPE expressed in FAP. Hum Gene. 1994;94:543-548.
- Traboulsi ET, Apostoides J, Giardiello FM, et al. Pigmented ocular fundus lesions and APC mutations in familial adenomatous polyposis. Ophth Genet. 1996;17:167-174.
- Deibert B, Ferris L, Sanchez N, Weishaar P. The link between colon cancer and congenital hypertrophy of the retinal pigment epithelium (CHRPE). Am J Ophthalmol Case Rep. 2019 Sep;15:100524.
- Nieuwenhuis MH, Vasen HF. Correlations between mutation site in APC and phenotype of familial adenomatous polyposis (FAP): a review of the literature. Crit Rev Oncol Hematol. 2007;61:153-161.

{kind=link}