

CASE REPORT
The patient, aged 66, was admitted because of the deterioration of vision in the right eye, which appeared in the last 2–3 months. The patient was pseudophakic in both eyes for 3 years. There were no other eye diseases or eye injuries in history.

The documentation provided by the patient proved recent several examinations of both fundi, and all of them were described as normal. The corrected visual acuity in the right eye was 0.3, and in the left eye −0.6.
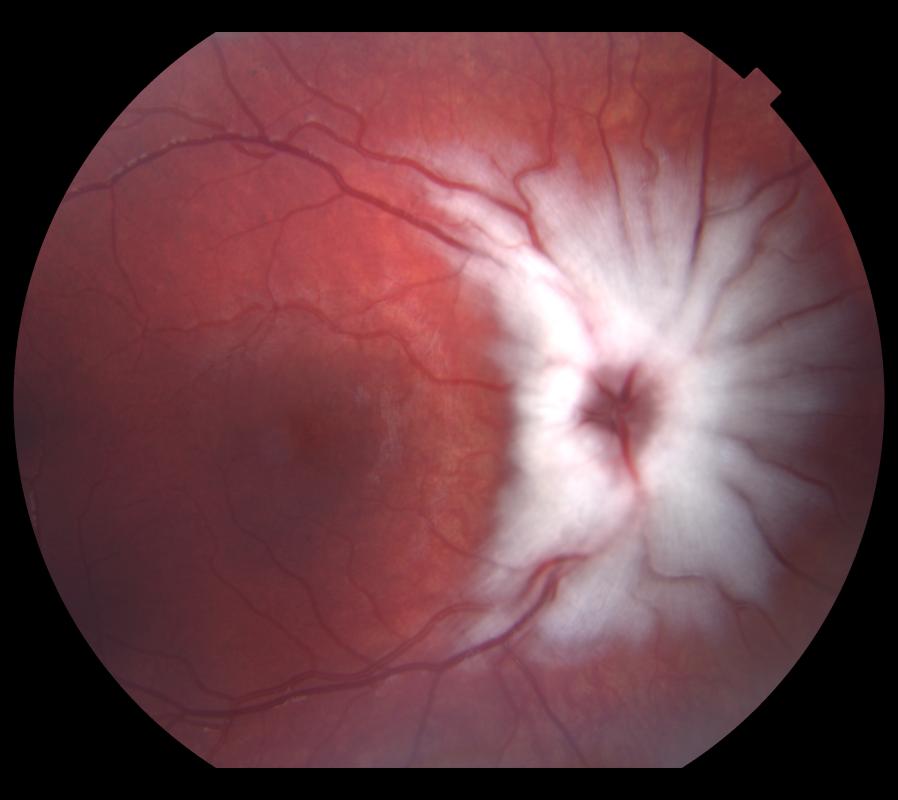
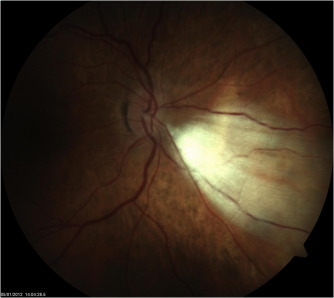
Physical examination revealed the posterior capsule opacification (PCO) in the right eye, white lesions on the retina of the right eye around the optic disk, and in the left eye – the peripheral, which could correspond to the myelinated fibers.
The patient claimed that she repeatedly went through a fundus examination and was never informed of the existence of such lesions. Visual fields showed defects corresponding to the MRNF of the retina in both eyes. OCT scans confirmed the typical picture of the Myelinated Retinal Nerve Fiber Layer (MRNF) around the optic disk in the right eye.
Myelinated Retinal Nerve Fiber Layer DISEASE entity
Myelinated Retinal Nerve Fiber Layer (MRNF) are retinal nerve fibers anterior to the lamina cribrosa that, unlike normal retinal nerve fibers, have a myelin sheath.

Clinically, they appear to be gray-white well-demarcated patches with frayed borders on the anterior surface of the neurosensory retina. MRNF are present in 0.57 to 1% of the population and can occur bilaterally in approximately 7% of affected patients.
Most patients with MRNF are asymptomatic; however, some patients have associated ocular findings including axial myopia, amblyopia, and strabismus. Though rare, familial cases of Myelinated Retinal Nerve Fiber Layer (MRNF) have been reported both in isolation and in combination with ocular and systemic syndromes.
MRNF are typically present at birth and are static lesions, but a few cases of acquired and progressive lesions in both childhood and adulthood have been described. The disappearance of MRNF has also been reported after surgery and insults to the optic nerve.
Myelinated Retinal Nerve Fiber Layer MANAGEMENT
Myelinated Retinal Nerve Fiber Layer (MRNF) is typically benign but can be mistaken for other potentially serious conditions. A complete blood count may be helpful when considering a neoplastic infiltrate.
The hyperreflectivity on OCT can mimic findings of retinal vascular occlusion or cotton wool spots, so ophthalmoscopy and fluorescein angiography can aid in distinguishing an embolic phenomenon.
In young children, extensive MRNF may be mistaken for retinoblastoma, which must be distinguished by careful ophthalmoscopy (often under anesthesia) and possible additional imaging, such as ocular ultrasound, OCT, and FAF.
If gross visual defects are present, formal visual field testing is warranted to rule out a concomitant neuro-ophthalmologic issue, as visual defects in MRNF are usually mild.
Management of MRNF is focused on serial eye examinations assessing for and treating associated conditions. Myopia should be treated with refractive correction. If significant anisometropia is present, correction with glasses may not be tolerated secondary to aniseikonia, and contact lenses should be prescribed.
Childhood amblyopia should be treated to optimize visual development. Strabismus should be managed with the usual protocols, and patients often respond well to surgical realignment.
It is important to recognize the generally benign nature of MRNF to avoid superfluous medical testing. It is helpful to document a MRNF with imaging as certain conditions can be associated with the loss of myelination, as described above.

Occasionally MRNF is referred for leukocoria. Careful observation of the feathering of the myelination along the nerve fiber layer can distinguish it from concerning diagnoses that can cause leukocoria, such as retinoblastoma.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Virchow VR. Zur pathologischen anatomic der netzaut und des scherven. Virchows Arch Pathol Anat. 1856;10:170–193.
- Gradle HS. The Blind Spot: III. The Relation of the Blind Spot to Medullated Nerve Fibers in the Retina. Journal of the American Medical Association. 1921;77(19):1483–7.
- Panigrahi A, Singh A, Gupta V. Syndrome of Myelinated Nerve Fibers, Hyperopia, Strabismus, and Amblyopia. Ophthalmol Retina. 2022 Dec;6(12):1153. doi: 10.1016/j.oret.2022.10.003. Epub 2022 Nov 4. PMID: 36344423.
- Kodama T, Hayasaka S, Setogawa T. Myelinated retinal nerve fibers: prevalence, location, and effect on visual acuity. Ophthalmologica. Journal international d’ophtalmologie. International Journal of Ophthalmology. Zeitschrift für Augenheilkunde. 1990;200(2):77–83. Available at: http://www.ncbi.nlm.nih.gov/pubmed/2338989. Accessed July 20, 2013.
- Straatsma BR, Foos RY, Heckenlively JR, Taylor GN. Myelinated retinal nerve fibers. American Journal of Ophthalmology. 1981;91(1):25–38. Available at: http://www.ncbi.nlm.nih.gov/pubmed/7234927. Accessed July 20, 2013.
- Funnell CL, George NDL, Pai V. Familial myelinated retinal nerve fibers. Eye (London, England). 2003;17(1):96–7. Available at: http://www.ncbi.nlm.nih.gov/pubmed/12579180. Accessed July 20, 2013.

{kind=link}