
CASE REPORT
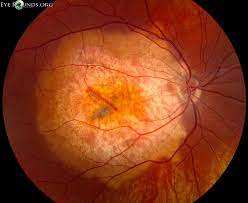
A 70-year-old man was referred to a clinic because of bilateral fundus lesions. He had a history of chronic kidney disease (CKD) and secondary hyperparathyroidism. Smartphone Fundoscopy showed a cluster of choroidal folds in the superotemporal extra-macular region OS.


Swept-source optical coherence tomography demonstrated ellipsoid zone disruption OD, retinal pigment epithelium undulation OS, dilated Haller layer veins OU, and central choroidal thickening OU and thinning of the overlying choroid due to scleral elevation OS.
Fluorescein angiography detected macular hyperfluorescence OD. Indocyanine green angiography demonstrated choroidal vascular hyperpermeability together with numerous scattered hypofluorescent lesions OU.
Fundus autofluorescence showed multiple hypoautofluorescent spots surrounded by hyperautofluorescent areas OD. Laser speckle flowgraphy exhibited choroidal blood flow reduction represented by a cold color pattern OU.
B-mode echography displayed hyperechoic solid lesions with acoustic shadowing and orbital computed tomography revealed high-density areas in the sclera, both of which were consistent with calcification. The patient was diagnosed with Sclerochoroidal Calcification.
Sclerochoroidal Calcification DISEASE entity
Sclerochoroidal calcification presents as flat or minimally elevated yellow placoid lesions, sometimes associated with gray lesions that are similar in appearance to senile scleral plaque. Sclerochoroidal Calcification is rare and frequently misdiagnosed.

The majority of cases are idiopathic and present with normal calcium-phosphorus metabolism and without associated ophthalmic or systemic conditions.
The majority of patients diagnosed with Sclerochoroidal Calcification are Caucasian and elderly. There is a slight female predisposition (approximately 60% of cases). Patients with previous systemic disorders that impact calcium-phosphorus metabolism are at higher risk of developing sclerochoroidal calcifications.
These include hyperparathyroidism, pseudohypoparathyroidism, parathyroid adenoma, chondrocalcinosis, sarcoidosis, Gitelman syndrome, Bartter syndrome, pseudo-gout, chronic renal disease, hypophosphatemia, hypervitaminosis, and metabolic imbalance after diuretic use.
Sclerochoroidal Calcification Symptoms
Patients are often asymptomatic and do not report ocular complaints. Patients do not typically show a change in visual acuity. However, there are several case reports of macular SCC associated with choroidal neovascularization or exudative retinal detachment resulting in decreased visual acuity.
However, a large review of 179 eyes of 118 patients did not report hemorrhage, subretinal fluid, retinal pigment epithelial detachment, or choroidal neovascular membrane (CNVM) in any case.
A long follow-up (mean 4 years) of these cases did not show enlargement of the lesion, hemorrhage, subretinal fluid, CNVM, vision loss, or decalcification. None of the cases needed treatment.

Diagnostic Procedures
Ophthalmoscopy ( Smartphone Fundoscopy ) is sufficient for diagnosis. The fellow eye may also have a similar and symmetrical lesion. There may be multiple lesions which, however, are typically localized near the superotemporal arcade or at the equator.
There might be atrophy of the overlying choroid and/or retinal pigment epithelium. The lesions may be arranged in a ring-like configuration. Calcifications can also be detected by B-scan ultrasonography, optical coherence tomography, orbital computed tomography, fundus autofluorescence, fluorescein angiography, and indocyanine green angiography.
Ophthalmoscopy can be unremarkable while ultrasound shows echogenic areas indicative of calcifications (hyperechoic lesion with acoustic shadow), due to deposition in the sclera not yet reaching the choroid.
Sclerochoroidal Calcification MANAGEMENT
General Treatment
Parathyroid adenoma, Bartter, and Gitelman syndromes should be ruled out with testing due to complications associated with these diseases.
Patients should be advised to return annually for a dilated eye exam to monitor the progression of the lesions, although there is no treatment other than correcting any metabolic imbalances.
Prognosis
Calcifications are commonly misdiagnosed, resulting in unnecessary testing and referral to retinal specialists.
Lesions are typically located away from the macula and rarely encroach the fovea, therefore visual prognosis in patients is good and visual acuity usually remains unchanged.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Honavar SG, Shields CL, Demirci H, & Shields JA. Sclerochoroidal calcification: clinical manifestations and systemic associations. Arch Ophthalmol. 2001;119(6), 833-840. doi:10.1001/archopht.119.6.833.
- Shields JA, Shields CL. CME Review: Sclerochoroidal calcification. Retina. 2002;22(3):251-261. doi:10.1097/00006982-200206000-00001.
- Shields CL, Hasanreisoglu M, Saktanasate J, Shields PW, Seibel I, Shields JA. Sclerochoroidal calcification. Retina. 2015;35(3):547-554. doi:10.1097/iae.0000000000000450.
- Thomson AC, Brown GT, Dolores-Rodriguez A, Hunter AA. A case of extensive bilateral idiopathic sclerochoroidal calcification and review of the literature. Int Med Case Rep J. 2021; 14:749-755. doi:10.2147/imcrj.s336237.
- Bourcier T, Blain P, Massin P, Grünfeld J-P, Gaudric A. Sclerochoroidal calcification associated with Gitelman syndrome. Am J Ophthalmol. 1999;128(6):767-768. doi:10.1016/s0002-9394(99)00277-9.
- Hasanreisoglu M, Saktanasate J, Shields PW, Shields CL. Classification of sclerochoroidal calcification based on enhanced depth imaging optical coherence tomography “mountain-like” features. Retina. 2015;35(7):1407-1414. doi:10.1097/iae.0000000000000468.

{kind=link}