
CASE REPORT
A 33-year-old woman was referred to an eye institute for a possible diagnosis of retinitis pigmentosa (RP). She reported decreased visual acuity for approximately the past 3 years and difficulty with night vision.


Cataracts were removed at the age of 33. Family history revealed that the proband’s father was diagnosed with RP at the age of 35 and her full brother had been diagnosed with RP at the age of 32. The proband’s paternal half-brother (age 31) reported night vision problems; however, he did not carry a definitive diagnosis.
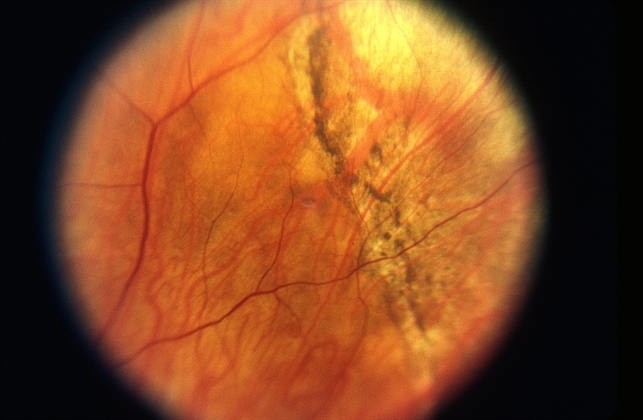
Smartphone fundoscopy showed generalized retinal pigment epithelial (RPE) atrophy with peripheral pigmentary changes OU. Retinal vessels were attenuated and optic discs were full with mild pallor OU. A vitreous veil was noted on examination OU.
Goldmann visual field (GVF) testing showed a markedly constricted central visual field OU. Spectral-domain optical coherence tomography (SD-OCT) showed cystoid macular edema (CME) OD and outer retinal disruption OU.
Both the scotopic and photopic full-field ERG were markedly abnormal OU confirming the diagnosis of Wagner Syndrome.
DISEASE
Wagner syndrome is an autosomal dominant vitreoretinopathy that results in a variety of ocular findings. The characteristic feature of the syndrome is an “optically empty” vitreous. Myopia, vitreous veils, presenile cataract, and night blindness are also commonly associated findings.

Wagner syndrome is caused by a mutation in the VCAN gene and is usually inherited in an autosomal dominant fashion but de novo cases have been reported.
MANAGEMENT
A baseline ophthalmological exam is required in patients diagnosed with Wagner syndrome to assess the extent of the disease. This should include best-corrected visual acuity, slit-lamp examination, measurement of intraocular pressure, and indirect ophthalmoscopy.
Ancillary testing should include visual field examination, Smartphone fundoscopy, optical coherence tomography, electroretinogram, and orthoptic assessment. Patients should also be referred to a clinical geneticist and/or a genetic counselor.
Children should also be monitored for amblyopia due to the high incidence of myopia in Wagner syndrome. In Wagner syndrome, the prevalence of retinal detachment (RD) is much higher but also significantly variable from family to family.

Rhegmatogenous retinal detachment (RRD) is the most common type of RD and its prevalence ranges from 6.3 to 17.9 per 100,000 subjects per year. In a follow-up of the original Swiss family, peripheral tractional RD was actually more commonly seen than RRD.
RRD was only reported in four eyes of four patients and occurred at an average age of 20 years, which was 14% of patients studied. Peripheral tractional RD was seen in 25% of all eyes and in 55% of the eyes of patients older than 45 years.
In the Japanese family studied by Miyamoto et al., RDs were observed in three eyes of three patients out of a total of eleven family members studied and one of these was a tractional RD. The age at which these RDs occurred was not specified.
However, in the French family studied by Brézin et al., nine out of twelve family members studied had RDs. These occurred primarily in childhood and adolescence, with the median age of occurrence being age 8. The earliest RD was observed at age 3 and the latest RD recorded was at age 33.
Medical therapy
Patients with Wagner syndrome should have an ophthalmologic examination annually by a vitreoretinal specialist. Glasses or contact lenses can be used to correct refractive errors.
Surgery
Surgical intervention in a patient with Wagner syndrome is much the same as in a patient without Wagner syndrome. Cataracts that cause significant impairment are removed and replaced with an intraocular lens implant.
Graemiger et al. suggests that cataract extraction be performed with extracapsular techniques to prevent the development of iris neovascularization and neovascular glaucoma.
They reported 20% of patients who had intracapsular cataract extraction developed iris neovascularization as compared to none who had extracapsular cataract extraction.
Laser retinopexy or cryotherapy can be used to treat retinal breaks without detachment. Retinal detachment, retinal traction involving the macula, or epiretinal membranes are indications for retinal surgery.
Most retinal detachments in Wagner syndrome are rhegmatogenous and repair is mainly focused on closing the retinal breaks via pars plana vitrectomy or retinal pneumopexy. Tractional retinal detachment is secondary to the shortening of the membranes connected to the retina.
Surgical repair of a tractional retinal detachment includes the removal of the membranes and vitreoretinal adhesions. Often, retinotomies are needed to relieve the traction.
Would you have interest in taking retina images by smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Kloeckener-Gruissem B, Amstutz C. VCAN-Related Vitreoretinopathy. GeneReviews® [Internet]. Adam MP, Ardinger HH, Pagon RA, et al., editors. Seattle (WA): University of Washington, Seattle; 1993-2020.
- Miyamoto T, Inoue H, Sakamoto Y, et al. Identification of a novel splice site mutation of the CSPG2 gene in a Japanese family with Wagner syndrome. Invest Ophthalmol Vis Sci. 2005;46(8):2726-2735. doi:10.1167/iovs.05-0057.
- Meredith SP, Richards AJ, Flanagan DW, Scott JD, Poulson AV, Snead MP. Clinical characterisation and molecular analysis of Wagner syndrome. Br J Ophthalmol. 2007;91(5):655-659. doi:10.1136/bjo.2006.104406.
- Brézin AP, Nedelec B, Barjol A, Rothschild PR, Delpech M, Valleix S. A new VCAN/versican splice acceptor site mutation in a French Wagner family associated with vascular and inflammatory ocular features. Mol Vis. 2011;17:1669-1678.
- Graemiger RA, Niemeyer G, Schneeberger SA, Messmer EP. Wagner vitreoretinal degeneration. Follow-up of the original pedigree. Ophthalmology. 1995;102(12):1830-1839. doi:10.1016/s0161-6420(95)30787-7.
- Keller KE, Kelley MJ, Acott TS. Extracellular matrix gene alternative splicing by trabecular meshwork cells in response to mechanical stretching. Invest Ophthalmol Vis Sci. 2007;48(3):1164-1172. doi:10.1167/iovs.06-0875.

{kind=link}