
DISEASE “Mooren’s Ulcer”
Mooren’s ulcer is characterized by painful peripheral corneal ulceration of unknown etiology. The disease generally begins with intense limbal inflammation and swelling in the episclera and conjunctiva.


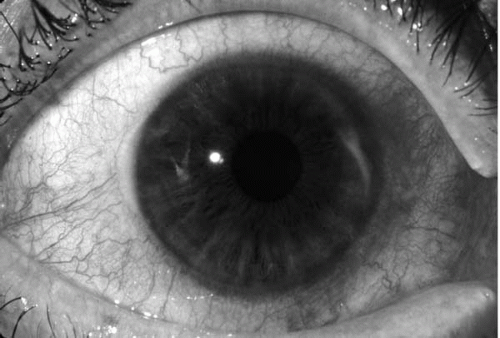
Corneal changes begin within 2-3 mm from the limbus, first appearing as grey swellings that rapidly furrow, affecting the superficial one-third of the cornea and then proceeding circumferentially and centrally over 4-12 months.
The bed of the furrow becomes vascularized, with vessels advancing into the base of the undermined edges of the ulcers. These ulcers are often described as crescent-shaped and can leave behind an opaque and edematous central cornea.
Alternatively,
they can completely consume the corneal stroma, replacing it with a thin fibrovascular membrane. Inflammation is not seen in the sclera adjacent to the peripheral ulcers, nor does it affect the underlying Descemet’s membrane.
Destruction of the cornea generally affects stromal tissue only, leaving behind an intact endothelium and epithelium.
The ulcer’s central edges can develop an overhanging edge with or without opacification, and cornea neovascularization can occur, extending from the limbus into the ulcer bed.
Neovascularization can occur up to the advancing edge of the ulcer but not beyond it.
Risk Factors of Mooren’s Ulcer
Risk factors for Mooren’s ulcer include corneal surgery, previous trauma, and infection. Although corneal surgery is a well-described risk factor, one study of 242 eyes affected by Mooren’s ulcer in South India described an interesting caveat.

An association has also been demonstrated between Mooren’s ulceration and hookworm infection. Certain helminths express receptors for calgranulin C, suggesting that there may be a helminthic antigen that cross-reacts with calgranulin C.
A previous infection has also been found to be a risk factor. An association with pyoderma gangrenosum has been described, implying potential common pathogenesis between the two processes since both pyoderma gangrenosum and Mooren’s ulcer show aseptic neutrophilic inflammation and both respond well to immunosuppression.
MANAGEMENT of Mooren’s Ulcer
Benign MU often doesn’t need to be treated if it doesn’t cause pain or doesn’t have any risk of complications.
If treatment is needed, both benign and malignant MU may be treated using one or more of the following:
- topical treatments to keep tissue from degenerating
- antibiotics, such as moxifloxacin (Vigamox), to prevent infections
- interferon a2b for hepatitis C infections, sometimes combined with the antiviral medication ribavirin (Rebetron)
- resection, or surgical removal of tissues surrounding the ulcer
- cryotherapy, which involves freezing and surgically removing ulcer tissue
- tissue adhesion, which involves placing materials near the ulcer to stop it from spreading
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- Watson, P.G., Management of Mooren’s ulceration. Eye (Lond), 1997. 11 ( Pt 3): p. 349-56.
- Chen, J., et al., Mooren’s ulcer in China: a study of clinical characteristics and treatment. Br J Ophthalmol, 2000. 84(11): p. 1244-9.
- Srinivasan, M., et al., Clinical characteristics of Mooren’s ulcer in South India. Br J Ophthalmol, 2007. 91(5): p. 570-5.
- Sangwan, V.S., P. Zafirakis, and C.S. Foster, Mooren’s ulcer: current concepts in management. Indian J Ophthalmol, 1997. 45(1): p. 7-17.
- Taylor, C.J., et al., HLA and Mooren’s ulceration. Br J Ophthalmol, 2000. 84(1): p. 72-5.
- Gottsch, J.D., et al., Cytokine-induced calgranulin C expression in keratocytes. Clin Immunol, 1999. 91(1): p. 34-40.
- Liang, C.K., et al., Association of HLA type and Mooren’s Ulcer in Chinese in Taiwan. Br J Ophthalmol, 2003. 87(6): p. 797-8.
Slit-lamp Smartphone photography

{kind=link}