
Modern vitreoretinal surgery has achieved remarkable success in the treatment of macular holes, epiretinal membranes, retinal detachments, diabetic tractional disease, and various complex retinal disorders.

Advances in instrumentation, visualization systems, and surgical techniques have significantly improved both anatomical and functional outcomes.
Despite these advances, vitreoretinal surgery is not without risks. One of the less common but potentially vision-threatening complications is the development of iatrogenic macular defects—retinal injuries occurring as an unintended consequence of surgical manipulation.
These defects may range from small inner retinal trauma to full-thickness macular holes and can adversely affect postoperative visual outcomes. Because they are relatively uncommon and often underrecognized, understanding their causes, risk factors, prevention, and management remains essential for retina specialists.
For vitreoretinal surgeons, awareness of iatrogenic macular defects is particularly important as surgical complexity continues to increase.
What Are Iatrogenic Macular Defects?
Iatrogenic macular defects are structural retinal abnormalities that develop during or shortly after vitreoretinal surgery as a direct result of surgical intervention.
They may involve:
- Inner retinal defects
- Dissociated retinal tissue changes
- Foveal trauma
- Lamellar macular holes
- Full-thickness macular holes
- Retinal thinning at manipulation sites
The severity ranges from clinically insignificant OCT findings to visually significant foveal damage.
👉 Not every postoperative macular abnormality represents disease progression; some may be procedure-related.
Why Do Iatrogenic Macular Defects Occur?
The macula is one of the most delicate structures in the eye.
Several surgical maneuvers may expose the retina to:
- Mechanical traction
- Instrument-induced trauma
- Excessive tissue manipulation
- Dye-related toxicity
- Shear stress during membrane peeling
Even technically successful surgery can occasionally result in microscopic retinal injury.
Common Types of Iatrogenic Macular Defects
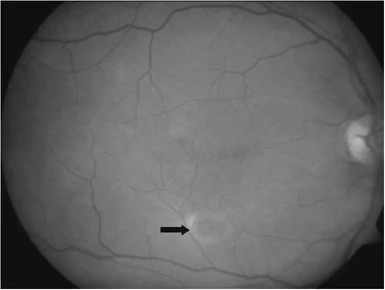
1. Iatrogenic Full-Thickness Macular Hole
Although uncommon, a full-thickness macular hole may develop after vitreoretinal surgery performed for unrelated conditions.
Associated Procedures
- Epiretinal membrane surgery
- Retinal detachment repair
- Diabetic vitrectomy
- Vitreomacular traction surgery
Proposed Mechanisms
- Excessive traction during membrane peeling
- Foveal tissue weakening
- Residual tangential traction
- Postoperative cystoid changes
👉 Secondary macular holes may appear days, weeks, or even months after surgery.
2. Inner Retinal Defects
These subtle abnormalities are increasingly recognized with high-resolution OCT.
Characteristics include:
- Localized retinal dimples
- Focal thinning
- Irregular inner retinal contour
They often occur following:
- Internal limiting membrane (ILM) peeling
- Extensive membrane dissection
Most are asymptomatic but may reflect microscopic surgical trauma.
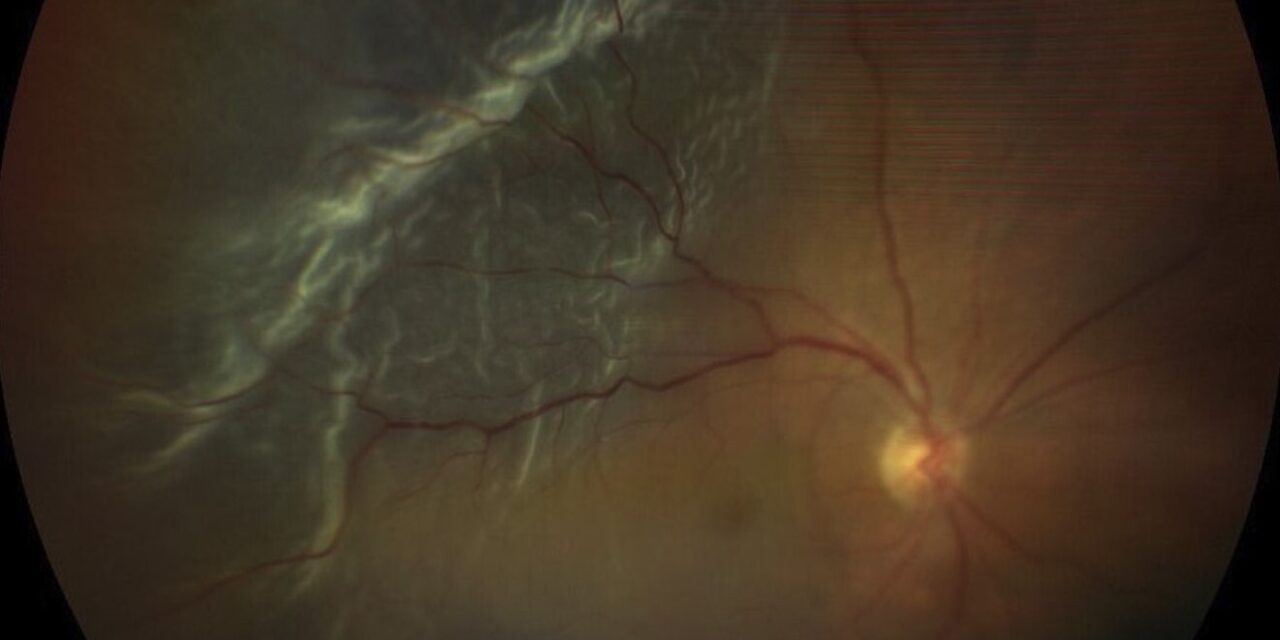
3. Dissociated Optic Nerve Fiber Layer (DONFL)
DONFL is a characteristic postoperative finding after ILM peeling.
OCT Appearance
- Small arcuate depressions
- Inner retinal dimpling
- Preservation of outer retinal layers
Clinical Significance
In most cases:
- Visual acuity remains unaffected
- No additional treatment is required
Although not considered a true complication by many surgeons, DONFL represents a form of surgically induced retinal alteration.
4. Iatrogenic Lamellar Macular Holes
Partial-thickness defects may occur when excessive traction is applied to fragile retinal tissue.
Risk factors include:
- Thin foveal tissue
- Pre-existing macular pathology
- Aggressive membrane peeling
Lamellar defects may remain stable or progress over time.
Surgical Factors That Increase Risk
1. Internal Limiting Membrane Peeling
ILM peeling has become a cornerstone of modern macular surgery.
Benefits include:
- Reduced recurrence of epiretinal membranes
- Improved macular hole closure rates
However, ILM peeling also introduces mechanical stress.
Potential consequences include:
- Müller cell injury
- Inner retinal trauma
- Retinal dimpling
👉 The therapeutic benefits of ILM peeling generally outweigh its risks, but careful technique remains essential.
2. Epiretinal Membrane Dissection
ERM removal may require significant tractional force.
Risk increases when:
- Membranes are densely adherent
- Visualization is poor
- Multiple grasping attempts are required
Excessive traction can result in focal retinal injury.
3. Forceps-Induced Trauma
Microforceps provide excellent control but can occasionally damage retinal tissue.
Potential injuries include:
- Direct retinal indentation
- Focal retinal tears
- Inner retinal defects
Modern small-gauge instrumentation has reduced these risks considerably.
4. Dye-Assisted Surgery
Vital dyes improve visualization of transparent tissues.
Common dyes include:
- Brilliant Blue G
- Trypan Blue
- Indocyanine Green (ICG)
Although generally safe, concerns remain regarding:
- Retinal toxicity
- Phototoxicity
- Dose-dependent cellular injury
👉 ICG has historically raised the greatest concerns regarding retinal toxicity.
5. Excessive Mechanical Manipulation
Repeated peeling attempts and prolonged surgery may increase cumulative retinal stress.
Factors include:
- Multiple membrane layers
- Difficult surgical planes
- Poor staining
- Limited visibility
The duration and complexity of surgery often correlate with injury risk.
Patient-Related Risk Factors
Certain retinal characteristics increase susceptibility to surgical injury.
High Myopia
Highly myopic eyes often exhibit:
- Thin retina
- Foveoschisis
- Posterior staphyloma
These structural changes increase vulnerability during peeling procedures.
Pre-Existing Macular Disease
Eyes with:
- Chronic epiretinal membranes
- Macular holes
- Cystoid macular edema
- Retinal atrophy
may possess weakened retinal architecture that is more susceptible to iatrogenic damage.
Advanced Age
Age-related retinal thinning and reduced tissue elasticity may contribute to increased fragility during surgery.
OCT: The Key to Detection
Many iatrogenic macular defects are invisible on clinical examination alone.
OCT Findings May Include
- Inner retinal dimples
- Focal retinal thinning
- Lamellar defects
- Full-thickness holes
- Disruption of retinal layers
Serial imaging is particularly useful for monitoring progression and assessing functional significance.
👉 OCT has dramatically improved recognition of subtle postoperative retinal changes.
Clinical Impact on Vision
The visual consequences depend on the location and severity of the defect.
Minimal Impact
Often seen with:
- DONFL
- Small inner retinal defects
- Peripheral macular changes
Significant Impact
More likely with:
- Foveal involvement
- Full-thickness macular holes
- Extensive retinal trauma
- Outer retinal disruption
Visual symptoms may include:
- Reduced acuity
- Metamorphopsia
- Central scotoma
- Reading difficulties
Prevention Strategies
Preventing iatrogenic macular defects begins with meticulous surgical technique.
Key Preventive Measures
Careful ILM Peeling
- Avoid excessive traction
- Use gentle peeling movements
- Maintain proper tissue planes
Optimal Visualization
- Adequate staining
- High-quality imaging systems
- Appropriate illumination
Minimize Retinal Grasping
- Reduce repeated forceps contact
- Use controlled movements
Patient Selection
Recognize high-risk eyes before surgery.
👉 Prevention is often more effective than managing established postoperative defects.

Management of Iatrogenic Macular Defects
Treatment depends on defect severity.
Observation
Appropriate for:
- DONFL
- Small inner retinal abnormalities
- Stable lamellar defects
Surgical Intervention
May be required for:
- Progressive lamellar holes
- Full-thickness macular holes
- Symptomatic tractional defects
Repeat vitrectomy, ILM flap techniques, and gas tamponade may be considered when necessary.
Future Perspectives
Technological advances continue to improve surgical safety.
Emerging innovations include:
- Intraoperative OCT
- Robotic-assisted vitreoretinal surgery
- Improved tissue visualization systems
- Safer staining agents
- Advanced retinal instrumentation
These developments may further reduce the incidence of surgically induced macular injury.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Pichi F, et al. “Retinal complications of internal limiting membrane peeling.” Retina. 2014.
- Tadayoni R, et al. “Dissociated optic nerve fiber layer appearance after internal limiting membrane peeling.” Ophthalmology. 2001.
- Steel DHW, Lotery AJ. “Retinal surface abnormalities after macular surgery.” Eye (Lond). 2013.
- Spaide RF. “Dissociated optic nerve fiber layer appearance and inner retinal dimpling after ILM peeling.” Retina. 2012.
- Shimada H, et al. “Secondary macular holes after vitrectomy.” Am J Ophthalmol. 2006.
- Haritoglou C, et al. “Indocyanine green-assisted peeling of the internal limiting membrane.” Am J Ophthalmol. 2003.

{kind=link}