
Introduction
Diabetic macular edema (DME) remains one of the leading causes of visual impairment among diabetic patients worldwide.

The introduction of anti-VEGF therapy revolutionized DME management, becoming the first-line treatment in most clinical scenarios.

However, despite regular injections and adherence to treatment protocols, a considerable proportion of patients demonstrate incomplete anatomical or functional response.
These cases are commonly referred to as resistant or persistent DME.
In recent years, corticosteroids have regained significant attention as an important therapeutic option in resistant DME.
Their ability to target inflammatory pathways involved in diabetic retinal disease offers a different mechanism of action compared to anti-VEGF agents.
Understanding when and how to use steroids appropriately is becoming increasingly important for retina specialists and comprehensive ophthalmologists alike.
Why Does DME Become Resistant?
DME is not solely a VEGF-driven disease. Although vascular endothelial growth factor plays a central role in vascular permeability, chronic diabetic retinal inflammation involves multiple cytokines and inflammatory mediators, including:
- Interleukins
- Tumor necrosis factor-alpha (TNF-α)
- Prostaglandins
- Adhesion molecules
This explains why some patients continue to exhibit persistent intraretinal or subretinal fluid despite repeated anti-VEGF injections.
Common Causes of Resistant DME:
- Chronic inflammatory component
- Delayed presentation with structural retinal damage
- Inadequate response to anti-VEGF therapy
- Poor systemic diabetic control
- Vitreomacular traction or epiretinal membrane
- Tachyphylaxis to anti-VEGF agents
👉 Resistant DME is generally considered when significant edema persists despite 3–6 consecutive anti-VEGF injections.
Why Steroids Work in DME
Corticosteroids address several inflammatory mechanisms simultaneously.
Their Main Actions Include:
- Stabilizing the blood-retinal barrier
- Reducing inflammatory cytokines
- Decreasing vascular permeability
- Inhibiting leukostasis
- Downregulating VEGF expression indirectly
Unlike anti-VEGF agents that target a single pathway, steroids act on multiple inflammatory cascades involved in chronic DME.
This makes them particularly useful in:
- Chronic DME
- Pseudophakic patients
- Inflammatory phenotypes of DME
- Cases with suboptimal anti-VEGF response
Available Steroid Options
1. Intravitreal Triamcinolone Acetonide (IVTA)
Triamcinolone was among the earliest steroids used for DME treatment.
Advantages:
- Relatively inexpensive
- Rapid edema reduction
- Useful in selected refractory cases
Limitations:
- Short duration of action
- Higher risk of intraocular pressure (IOP) elevation
- Cataract progression
Although less commonly used today compared to implants, IVTA remains valuable in resource-limited settings.
2. Dexamethasone Intravitreal Implant
The dexamethasone implant provides sustained steroid release over several months.
Advantages:
- Longer duration of action
- Strong anti-inflammatory effect
- Useful in vitrectomized eyes
- Reduced injection burden
Ideal Candidates:
- Resistant DME
- Pseudophakic patients
- Patients unable to maintain frequent follow-ups
- Patients with cardiovascular contraindications to anti-VEGF therapy
Several studies have demonstrated significant anatomical improvement with dexamethasone implants, especially in chronic DME.
3. Fluocinolone Acetonide Implant
This long-acting implant provides steroid delivery for up to several years.
Advantages:
- Extended control of chronic edema
- Reduced treatment frequency
Concerns:
- Higher cumulative risk of glaucoma
- Cataract formation
Therefore, careful patient selection is essential.
When Should Steroids Be Considered?
The timing of switching to steroids remains debated, but several practical indicators support their use.
Clinical Situations Favoring Steroids:
- Persistent edema after multiple anti-VEGF injections
- Chronic DME with inflammatory biomarkers on OCT
- Pseudophakia
- Poor compliance with monthly visits
- History of recent cardiovascular events
- Vitrectomized eyes
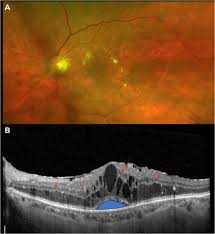
OCT Features Suggestive of Better Steroid Response:
- Hyperreflective retinal foci
- Subretinal fluid
- Large intraretinal cysts
These findings may indicate a stronger inflammatory component.
Steroids vs Anti-VEGF: Is It a Competition?
The question is not whether steroids are better than anti-VEGF agents overall, but rather which patients benefit most from each therapy.
Anti-VEGF Therapy Remains First-Line Because:
- Better visual outcomes in many treatment-naïve cases
- Lower risk of cataract progression
- Safer long-term IOP profile
Steroids Become Valuable When:
- Anti-VEGF response is inadequate
- Inflammation plays a larger role
- The injection burden becomes problematic
In many real-world cases, a tailored combination or sequential strategy may provide the best outcomes.
Complications and Monitoring
Steroids are highly effective, but they are not without risks.
Major Complications:
- Elevated intraocular pressure
- Steroid-induced glaucoma
- Cataract progression
- Rare risk of infection
Monitoring Recommendations:
- Regular IOP checks
- Lens status assessment
- OCT monitoring for recurrence
👉 Patients with pre-existing glaucoma require careful evaluation before steroid use.
Future Perspectives
Emerging research suggests that personalized DME treatment may become increasingly important. Instead of applying the same treatment algorithm to every patient, clinicians may soon rely on:
- OCT biomarkers
- Artificial intelligence analysis
- Cytokine profiling
- Individual inflammatory signatures
This could help identify patients who would benefit from early steroid therapy rather than prolonged ineffective anti-VEGF treatment.
Conclusion
Steroids play a critical and expanding role in the management of resistant diabetic macular edema.
By targeting the inflammatory component of DME, they provide an effective alternative for patients with inadequate anti-VEGF response, chronic edema, or high treatment burden.
Successful use of steroids depends on:
- Proper patient selection
- Careful monitoring
- Understanding the balance between efficacy and side effects
In the era of personalized retina care, steroids are no longer considered merely second-line rescue therapy—they are becoming an essential part of the modern DME treatment strategy.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Diabetic Retinopathy Clinical Research Network (DRCR.net). “Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus laser for diabetic macular edema.” Ophthalmology. 2010.
- Boyer DS, et al. “Dexamethasone intravitreal implant for treatment of diabetic macular edema.” Ophthalmology. 2014.
- Gillies MC, et al. “Intravitreal triamcinolone for refractory diabetic macular edema.” Ophthalmology. 2006.
- Schmidt-Erfurth U, et al. “Guidelines for the management of diabetic macular edema.” Acta Ophthalmologica. 2017.
- Korobelnik JF, et al. “Intravitreal aflibercept for diabetic macular edema.” Ophthalmology. 2014.
- Campochiaro PA, et al. “Sustained delivery fluocinolone acetonide vitreous inserts provide benefit for at least 3 years in patients with diabetic macular edema.” Ophthalmology. 2012.

{kind=link}