

Case Presentation
A 28-year-old male presented to the emergency department with sudden vision loss in the right eye following a high-velocity pellet gun injury to the face 12 hours prior.

He reported an immediate decrease in vision after the incident, with no prior ocular history or systemic comorbidities.
Examination revealed visual acuity of counting fingers in the right eye and 20/20 in the left, intraocular pressure of 14 mmHg bilaterally, conjunctival chemosis and subconjunctival hemorrhage inferonasally in the right eye.
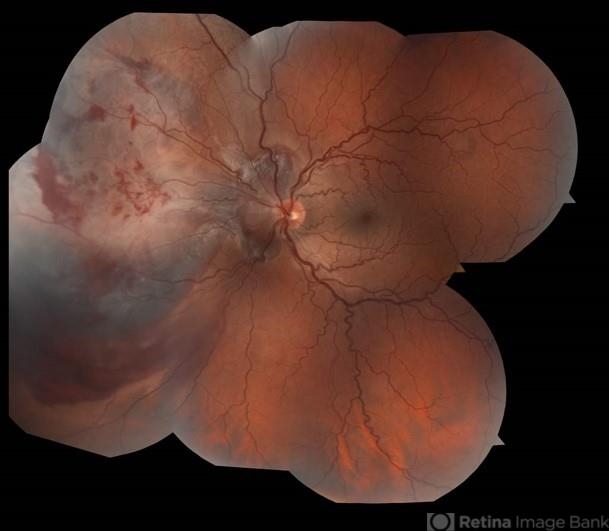
A clear anterior segment, dense vitreous hemorrhage obscuring fundus details, and orbital computed tomography showing a medial wall fracture with the projectile in the sphenoid sinus, but no intraocular foreign body. A diagnosis of Retinitis Sclopetaria was made.
Disease Entity
Retinitis sclopetaria, also termed chorioretinitis sclopetaria, represents a distinctive form of traumatic chorioretinal rupture.
High-velocity projectiles passing adjacent to the globe generate shock waves that disrupt the choroid, retinal pigment epithelium, Bruch membrane, and neurosensory retina.
Ophthalmologists must recognize this entity promptly. It demands differentiation from other posterior segment traumas.
Misdiagnosis risks inappropriate intervention. The condition carries implications for long-term visual function and secondary complications.
This injury underscores the need for vigilant post-traumatic monitoring. It highlights mechanical tissue disparities in ocular layers. Clinicians encounter it in trauma settings, particularly penetrating or blunt high-energy events.
Pathophysiology
The mechanism initiates with a high-velocity projectile grazing the orbit. This creates a shock wave that transmits compressive forces to ocular tissues.
Sclera and neurosensory retina exhibit high elasticity. They retract without full-thickness rupture. In contrast, Bruch membrane, choriocapillaris, and retinal pigment epithelium prove inelastic.
These rigid layers rupture first. Subretinal and intraretinal hemorrhages ensue rapidly. Vitreous hemorrhage often overlies the site.
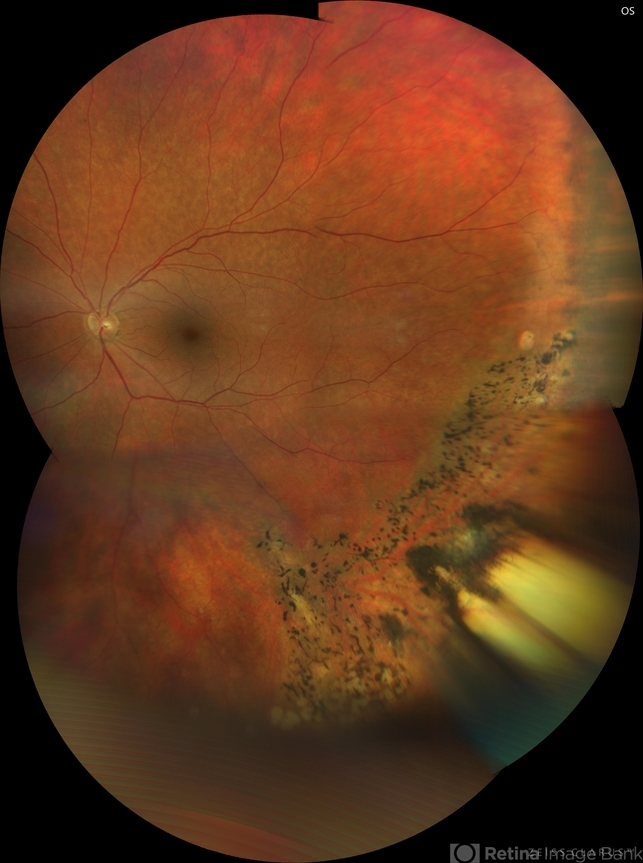
Tissue retraction exposes bare sclera initially. Hemorrhage organizes over days to weeks. Fibrovascular proliferation bridges the defect.
Retinal pigment epithelium hyperplasias. Dense retinal fibrosis fuses with choroidal scarring. This anchors the retina, minimizing acute detachment risk.
Photoreceptor loss predominates in affected zones. Ganglion cell layer cellularity declines. Macular involvement amplifies damage.
Late sequelae include fibrous scars with irregular, serrated borders. Claw-like configurations emerge. Glial proliferation stabilizes the rupture site.
Epidemiology
Retinitis sclopetaria affects predominantly young adults. Typical age ranges from 20 to 40 years. Pediatric cases occur but remain less common.
Males predominate significantly. This reflects higher exposure to high-velocity projectile risks, such as firearms or pellet guns.
Risk factors center on trauma mechanisms. High-velocity missiles adjacent to the globe prove essential. Gunshot wounds, BB pellets, and air rifle injuries predominate.
Urban violence contributes to the rising incidence. Recreational shooting accounts for many cases. No strong genetic or systemic predispositions exist.
Bilateral involvement proves rare. Unilateral presentation characterizes nearly all instances.

Clinical Features
- Patients report acute vision loss post-trauma, often unilateral.
- Symptoms include blurred vision, floaters from vitreous hemorrhage, and photopsia.
- Onset occurs immediately after injury, with progression over hours to days as hemorrhage settles.
- Pain manifests rarely unless an associated orbital fracture exists.
- Redness and irritation arise from conjunctival involvement.
- Progression features hemorrhage resorption, followed by scar formation over weeks.
- Unilateral involvement predominates; bilateral cases link to massive trauma.
- Macular lesions yield central scotomas; peripheral sites cause field defects.
Examination Findings
- Visual acuity varies widely: counting fingers to 20/200 common acutely, and potential improvement to 20/60 with foveal sparing.
- Relative afferent pupillary defect appears in severe cases.
- Anterior segment shows chemosis, subconjunctival hemorrhage, and occasional hyphema.
- Fundus reveals broad whitening, bare sclera exposure inferonasally or temporally, and intraretinal and preretinal hemorrhages.
- Vitreous hemorrhage obscures views initially, and clears gradually.
- Optical coherence tomography demonstrates choroidal rupture, outer retinal defects, photoreceptor loss, and subretinal fibrosis.
- Fluorescein angiography shows early hypofluorescence and late staining of scars without leakage.
- B-scan ultrasonography confirms retinal attachment, choroidal thickening, and no foreign bodies.
- Computed tomography identifies orbital fractures, projectile location, and excludes intraocular metal.
Differential Diagnosis
- Commotio retinae: transient whitening without rupture or bare sclera.
- Choroidal rupture: linear lesions without retinal/choroidal gaping.
- Retinal detachment: elevated retina, no fibrotic bridging.
- Berlin edema: macular whitening post-blunt trauma, resolves quickly.
- Traumatic macular hole: central full-thickness defect.
- Penetrating globe injury: intraocular foreign body, full-thickness laceration.
- Posterior uveitis: inflammatory signs, bilateral potential.
- Choroidal neovascularization: late post-trauma, leakage on angiography.
Diagnosis
Clinicians establish diagnoa sis clinically via trauma history and characteristic fundus findings. Bare sclera with surrounding hemorrhage and whitening confirms the entity.
Imaging plays a pivotal role. Orbital computed tomography rules out foreign bodies and fractures. B-scan ultrasonography assesses attachment and vitreous status.
Optical coherence tomography delineates layer-specific disruptions. Fluorescein angiography characterizes perfusion and scarring.
Ancillary tests include gonioscopy for angle recession. Electrophysiology aids prognosis in opaque media.
No laboratory workup proves routine absent infection suspicion.
Management
Observation
The primary approach favors close observation. Acute retinal detachment risk stays low due to fibrotic adhesion. Monitor weekly initially for hemorrhage clearance.
Serial examinations track scar evolution. Laser prophylaxis is avoided due to poor outcomes.
Medical Treatment
Topical corticosteroids reduce inflammation. Prednisolone acetate 1% every 2 hours tapers over weeks. Cycloplegics like scopolamine manage pain.
Antibiotics prevent endophthalmitis if penetration is suspected. Systemic steroids are considered for optic neuropathy.
Evidence supports conservative initial care. Surgery is reserved for complications.
Surgical Treatment
Indications include non-clearing vitreous hemorrhage, late retinal detachment, or epiretinal membranes. Pars plana vitrectomy clears the media.
Scleral buckling is applied rarely for peripheral breaks. Endolaser and tamponade secure repairs.
Immediate surgery lacks benefit over observation. Multivariate analyses show no visual acuity advantage.
Prognosis
Visual outcomes prove guarded. Most achieve 20/200 or worse. Favorable cases reach 20/60 with peripheral lesions.
Prognostic factors include macular involvement, temporal location, and early foreign body removal. Foveal sparing predicts better recovery.
Traumatic optic neuropathy limits gains. Photoreceptor loss persists indefinitely.
Follow-up requires lifelong monitoring. Quarterly visits assess for delayed hemorrhage, detachment, or neovascularization initially, then biannually.
Prevention (if applicable)
Target risk factor control through firearm safety education. Promote protective eyewear in shooting sports.
Screen high-risk populations like young males in urban areas. Public health campaigns reduce recreational projectile injuries.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
1. University of Iowa Eye Forum. Chorioretinitis Sclopetaria: A Systems-Based Approach to Eye Injury.
2. Kuhn F, et al. Treatment and pathogenesis of traumatic chorioretinal rupture (sclopetaria). Ophthalmology. 1994.
3. American Journal of Ophthalmology. Traumatic chorioretinitis sclopetaria: Risk factors, management, and prognosis. 2019.
4. Retina Today. Bullet Proof: A Case of Chorioretinitis Sclopetaria. 2024.
5. Ryan’s Retina. Traumatic Chorioretinal Injuries. 7th Edition.

{kind=link}