

Case Study
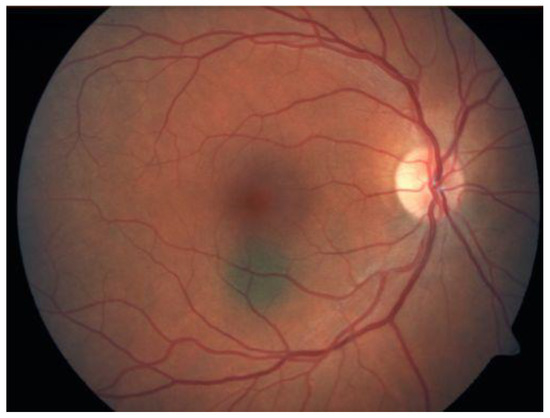
A 56-year-old woman presented with a pigmented lesion in the posterior pole of her left eye, discovered incidentally during a routine ophthalmic examination.


She had no visual complaints, and her best-corrected visual acuity was 20/20 in both eyes. Fundus examination revealed a dark brown, dome-shaped lesion at the peripapillary region with well-defined margins.
Optical coherence tomography (OCT) demonstrated a mildly elevated lesion with intact overlying retina, while B-scan ultrasonography showed medium internal reflectivity.
Given the lesion’s appearance, a differential diagnosis including choroidal melanoma was considered.
However, long-term observation revealed no growth, confirming the diagnosis of Choroidal Melanocytoma—a benign but deceptively pigmented tumor.
Disease Entity
Choroidal Melanocytoma is a rare, benign pigmented tumor of the uveal tract, typically composed of deeply pigmented melanocytes.
Although histologically benign, its clinical presentation can mimic malignant melanoma, making accurate differentiation essential to avoid unnecessary enucleation.
It most commonly affects the optic disc or peripapillary region, but can occasionally arise in the choroid or ciliary body.
Pathophysiology
Choroidal melanocytomas arise from melanocytes—neural crest-derived cells responsible for ocular pigmentation.
These lesions consist of round or polygonal cells containing abundant melanin granules that can obscure nuclear details.
Despite being benign, they may undergo necrosis or cause secondary inflammation, leading to local complications such as vitreous seeding or retinal edema.
Rarely, transformation into malignant melanoma has been reported, though this remains exceedingly uncommon.
Epidemiology
Choroidal melanocytoma is most frequently diagnosed in middle-aged adults, with a slight predilection for females. There appears to be no racial predilection, although darker-skinned individuals may have a higher incidence of ocular melanocytic lesions in general.
The optic disc is the most common site of involvement, followed by the peripapillary choroid.
Clinical Features
Patients are often asymptomatic, and the lesion is usually discovered incidentally.
When symptomatic, visual disturbance may result from compression of the optic nerve, secondary serous retinal detachment, or vitreous seeding.
Typical clinical findings include:
-
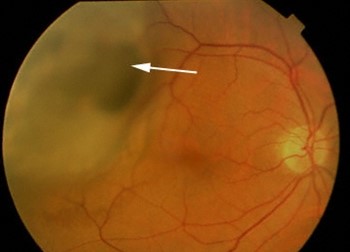
A dark brown to black, elevated mass on the optic disc or adjacent choroid
-
Sharp, well-defined margins
-
Occasional orange pigmentation or mottling due to necrosis
-
Overlying retinal edema or subretinal fluid in symptomatic cases
Examination Findings
-
Fundus Examination: Deeply pigmented, dome-shaped lesion with sharp borders and occasional overlying exudation.
-
OCT: Localized elevation with intact retinal layers, sometimes showing subretinal fluid.
-
B-scan Ultrasonography: Medium internal reflectivity (distinguishing it from the low reflectivity of melanoma).
-
Fluorescein Angiography: Hypofluorescence throughout, as dense melanin blocks fluorescence.
-
Autofluorescence Imaging: Hypoautofluorescent due to heavy pigmentation.
Differential Diagnosis
Because of its pigmentation and elevation, Choroidal Melanocytoma can easily be mistaken for:
-
Choroidal melanoma – tends to show orange pigment, lipofuscin, and low internal reflectivity
-
Choroidal nevus – typically flat or slightly elevated with less dense pigmentation
-
Adenoma of the retinal pigment epithelium (RPE) – may have irregular margins and less pigmentation
-
Optic disc melanoma or metastasis – often accompanied by rapid growth and visual symptoms
Diagnosis
Diagnosis is based primarily on characteristic clinical and imaging findings. Stability over time is the key diagnostic indicator confirming benignity.
-
Observation: Most lesions are monitored with periodic fundus photography and OCT to document stability.
-
Fine-needle aspiration biopsy (FNAB): Rarely indicated, reserved for cases where malignancy cannot be excluded through imaging alone.
Management
Observation is the mainstay of management for choroidal melanocytoma. Regular follow-up every 6–12 months is recommended to detect any signs of growth or complications.
-
Indications for intervention:
-
Documented lesion enlargement
-
Secondary complications such as vitreous seeding or retinal detachment
-
Diagnostic uncertainty
-
-
Treatment options:
-
Laser photocoagulation or radiotherapy in selected cases with exudative complications
-
Enucleation only if malignant transformation or extensive necrosis is confirmed
-
Prognosis
The prognosis for choroidal melanocytoma is excellent in most cases, as these tumors remain stable for years or decades.
However, patients should be educated about the importance of follow-up, since complications such as necrosis, inflammation, or rare malignant transformation can alter outcomes.
Vision may be affected if the lesion involves the optic disc or causes secondary retinal damage.
Prevention
There are no established preventive measures, as choroidal melanocytoma is a sporadic condition without known modifiable risk factors.
However, early detection and regular ophthalmic evaluations are crucial for differentiation from more aggressive lesions.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
-
Shields JA, Shields CL. Intraocular Tumors: An Atlas and Textbook, 3rd Edition. Lippincott Williams & Wilkins; 2016.
-
Arepalli S, Kaliki S, Shields CL. Choroidal melanocytoma: Clinical features and natural course in 115 cases. Br J Ophthalmol. 2015;99(3):377–382.
-
Singh AD, Damato BE, Pe’er J, et al. Clinical Ophthalmic Oncology: Uveal Tumors. Springer; 2019.
-
Demirci H, Shields CL, Eagle RC Jr. Choroidal melanocytoma: Clinicopathologic correlation in 17 cases. Arch Ophthalmol. 2001;119(12):1767–1774.

{kind=link}