
Disease Entity
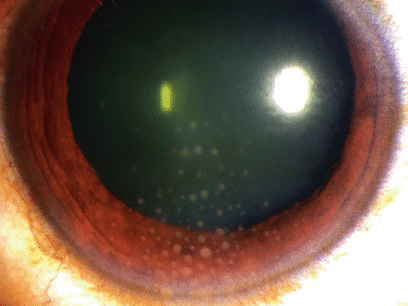
Arlt’s triangle is a specific pattern of keratic precipitates (KPs) distributed as an inverted triangle on the inferior corneal endothelium.


These precipitates, often greasy and white-yellowish, consist of macrophages and epithelioid cells and are characteristic of granulomatous anterior uveitis.
While not pathognomonic of a particular etiology, this clinical finding often points to chronic inflammatory or infectious processes such as sarcoidosis, tuberculosis, or syphilis.
Effective management of Arlt’s triangle requires addressing the underlying cause, controlling inflammation, and preventing complications such as posterior synechiae, secondary glaucoma, or permanent endothelial damage.
For an in-depth understanding of the causes and diagnostic approach to Arlt’s Triangle, refer to the original article here.
Management Strategies
1. General Principles of Management
The treatment of Arlt’s triangle focuses on controlling the inflammation in the anterior chamber, treating any underlying systemic or infectious causes, and mitigating potential complications.
Management typically involves a combination of pharmacological therapies and, in some cases, surgical intervention. Below are the detailed steps for managing this condition:
Cycloplegic Agents
- Purpose: Cycloplegic drugs are used to relieve pain from ciliary spasms and to prevent or break posterior synechiae.
- Common Agents:
- Cyclopentolate: A medium-acting agent often preferred for acute cases.
- Homatropine: Provides longer-lasting cycloplegia for chronic inflammation.
- Atropine: Used in severe cases to ensure maximal cycloplegia and mydriasis.
- Duration of Use: Cycloplegics are administered until the inflammation subsides and the risk of synechiae formation is mitigated.
Topical Corticosteroids
- Purpose: To suppress the inflammatory response in the anterior chamber.
- Commonly Used Steroids:
- Prednisolone acetate 1%: A first-line choice for its potent anti-inflammatory effects.
- Difluprednate: A more potent alternative often used for severe cases.
- Frequency: Typically administered every 1-2 hours during the acute phase and gradually tapered as inflammation subsides.
- Monitoring: Prolonged use requires monitoring intraocular pressure (IOP) to prevent steroid-induced glaucoma.

Subconjunctival Corticosteroid Injections
- Indications:
- For patients who are non-compliant with topical therapy.
- When topical steroids fail to control inflammation.
- Agents:
- Triamcinolone acetate: Provides long-lasting effects but should be avoided in infectious uveitis.
- Betamethasone: A shorter-acting option used in acute exacerbations.
- Precautions: Careful consideration is needed to rule out infectious causes before administration.
Oral Corticosteroids
- Indications:
- Severe or bilateral inflammation.
- Associated systemic inflammatory or autoimmune disease.
- Typical Regimen:
- Prednisone 40-60 mg/day initially, tapered based on response.
- Adjunct Therapy:
- Concomitant prophylactic therapy against gastric ulcers (e.g., proton pump inhibitors) and osteoporosis (e.g., calcium and vitamin D supplements).
Non-steroidal anti-inflammatory Drugs (NSAIDs)
- Use: For mild to moderate cases where corticosteroids are contraindicated or as an adjunct therapy in chronic uveitis.
- Examples: Topical diclofenac or ketorolac.
2. Infectious Causes and Specific Therapies
If the inflammation is caused by an infectious etiology, targeted antimicrobial therapy is critical:
Tuberculosis (TB)
- Management:
- Combination therapy with isoniazid, rifampin, ethambutol, and pyrazinamide.
- Corticosteroids may be used concurrently to control inflammation.
- Monitoring: Regular liver function tests and follow-up imaging.
Syphilis
- Management:
- Intravenous penicillin G remains the standard of care.
- Alternative regimens include ceftriaxone or doxycycline for penicillin-allergic patients.
Herpes Simplex Virus (HSV) or Varicella Zoster Virus (VZV)
- Management:
- Oral antiviral agents like acyclovir, valacyclovir, or famciclovir.
- Topical antivirals (e.g., ganciclovir gel) may be used adjunctively.
Toxoplasmosis
- Management:
- Triple therapy with pyrimethamine, sulfadiazine, and folinic acid.
- Clindamycin or azithromycin may be used in sulfadiazine-intolerant patients.
Fungal Infections (e.g., Coccidioidomycosis)
- Management:
- Systemic antifungals like voriconazole or amphotericin B.
3. Immune-Modulating Therapies
- Indications: Chronic or refractory cases, particularly in non-infectious etiologies such as sarcoidosis, Vogt-Koyanagi-Harada disease, or sympathetic ophthalmia.
- Common Agents:
- Methotrexate.
- Azathioprine.
- Mycophenolate mofetil.
- Biologics (e.g., adalimumab or infliximab for severe cases).
- Monitoring: Regular blood work to assess for drug toxicity and immunosuppression.
4. Management of Complications
Posterior Synechiae
- Early intervention with cycloplegics and frequent corticosteroids is essential to prevent or break adhesions.
- Surgical synechiolysis may be required in severe cases.
Secondary Glaucoma
- Management:
- Topical IOP-lowering agents (e.g., beta-blockers, carbonic anhydrase inhibitors).
- Avoid prostaglandin analogs, which may exacerbate inflammation.
- Surgical options like trabeculectomy or tube shunts for refractory cases.
Corneal Endothelial Damage
- Management:
- Monitor endothelial cell density.
- Consider keratoplasty if severe decompensation occurs.
5. Adjunctive Therapies
Lifestyle Modifications
- Advise patients to avoid triggers such as stress, systemic infections, and non-adherence to therapy.
Patient Education
- Emphasize the importance of follow-up care and adherence to prescribed therapies.
- Educate on recognizing signs of worsening inflammation or complications.
Conclusion
The management of Arlt’s triangle involves a multifaceted approach tailored to the underlying etiology and severity of inflammation.
By combining cycloplegia, corticosteroids, targeted antimicrobial therapies, and immune-modulating agents when necessary, ophthalmologists can effectively control inflammation, prevent complications, and improve patient outcomes.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Am J Ophthalmol. 2005;140(3):509-516. doi:10.1016/j.ajo.2005.03.057.
- Kim SJ, Yu YS. Diagnosis and treatment of anterior uveitis: clinical perspectives. Ocul Immunol Inflamm. 2010;18(1):33-39. doi:10.3109/09273940903493140.
- Rosenbaum JT, Dick AD, Anderson LC, et al. Insights into uveitis from an animal model and therapeutic implications. J Autoimmun. 2015;62:90-96. doi:10.1016/j.jaut.2015.05.001.
- Herbort CP, Rao NA, Mochizuki M. International criteria for the diagnosis of Vogt-Koyanagi-Harada disease: report of an international workshop on VKH. Am J Ophthalmol. 2001;131(5):647-652. doi:10.1016/s0002-9394(01)00842-9.
- Levy-Clarke G, Jabs DA, et al. Expert panel recommendations for the use of immunomodulatory agents in patients with ocular inflammatory disorders. Ophthalmology. 2014;121(3):785-796. doi:10.1016/j.ophtha.2013.11.026.
- Forrester JV, Dick AD, McMenamin PG, et al. The Eye: Basic Sciences in Practice. 4th ed. Elsevier; 2016. Chapter on anterior uveitis.

{kind=link}