
Case study
A 45-year-old woman with a history of congenital aniridia underwent bilateral implantation of a black diaphragm intraocular lens (IOL) to manage her photophobia and cosmetic concerns.

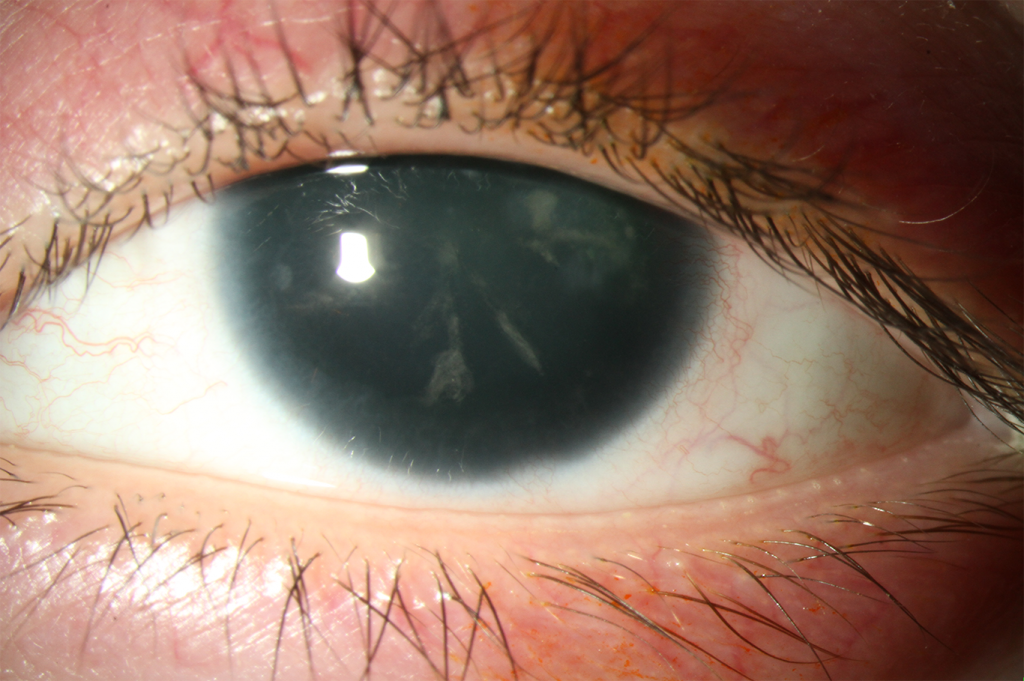
Over a decade post-surgery, she presented with progressive vision loss, ocular discomfort, and persistent redness in her left eye.
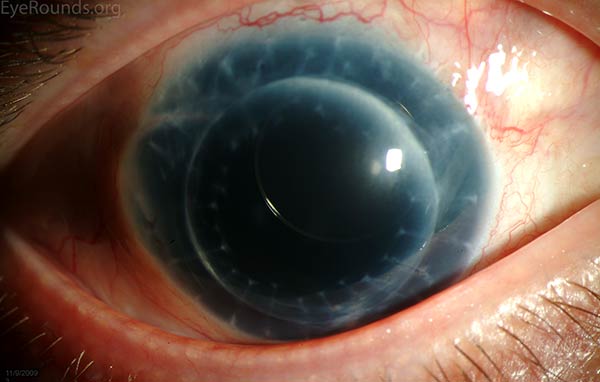
Examination revealed extensive fibrotic membranes forming over the anterior segment structures, including the IOL, iris remnants, and corneal endothelium.
Gonioscopy demonstrated peripheral anterior synechiae and closure of the angle. Surgical removal of the fibrotic tissue was attempted, but recurrent fibrosis complicated the postoperative course.
The patient was eventually managed with long-term intraocular pressure control and symptomatic treatment.
Disease entity
Aniridic Fibrosis Syndrome is a rare, progressive condition observed in patients with congenital aniridia, typically following surgical implantation of an intraocular lens (IOL).
This condition involves the proliferation of fibrotic tissue across the anterior segment structures, leading to complications such as synechiae, angle closure, and secondary glaucoma.
The syndrome reflects the underlying molecular and cellular abnormalities in congenital aniridia, particularly the role of PAX6 gene mutations, which affect ocular surface healing and cellular function.
Recognizing and managing this challenging complication is critical to preserving vision and maintaining ocular integrity.
Pathophysiology
Aniridic Fibrosis Syndrome is thought to arise from abnormal wound healing and cellular proliferation in the anterior segment of the eye.
Patients with congenital aniridia often have defective ocular surface development due to PAX6 gene mutations.
These mutations impair the regulation of cell proliferation and differentiation, leading to aberrant fibrovascular tissue growth. Surgical trauma, particularly during or after IOL implantation, can trigger a cascade of inflammatory and fibrotic responses, causing excessive extracellular matrix deposition.
Over time, this leads to adhesion of anterior segment structures and progressive fibrosis.
Epidemiology
- Aniridic Fibrosis Syndrome is primarily observed in patients with congenital aniridia who have undergone anterior segment surgery, especially IOL implantation.
- The syndrome is rare but may be underreported due to its variable presentation and delayed onset.
- It is more prevalent in cases where aniridic IOLs are implanted, as these lenses may exacerbate the fibrotic response.
Clinical Features
The clinical presentation of Aniridic Fibrosis Syndrome varies, but common findings include:
- Fibrotic Membranes: Proliferation of fibrous tissue over the iris, IOL, or corneal endothelium.
- Progressive Vision Loss: Due to obstruction of the visual axis and secondary complications.
- Elevated Intraocular Pressure (IOP): Secondary glaucoma may develop from angle closure or fibrosis-related outflow obstruction.
- Ocular Discomfort: Persistent redness and irritation are common.

Examination Findings
- Slit-Lamp Examination: Thick fibrotic membranes covering the anterior segment.
- Gonioscopy: Peripheral anterior synechiae, angle closure, and scarring.
- Ultrasound Biomicroscopy (UBM): Assessment of fibrotic tissue involvement in deeper anterior segment structures.
Differential Diagnosis
- Ocular cicatricial pemphigoid
- Postoperative anterior segment fibrosis
- Epithelial downgrowth
- Iridocorneal endothelial syndrome
- Traumatic fibrotic membranes
Diagnosis
The diagnosis is clinical and based on history, examination findings, and imaging studies:
- History of congenital aniridia and anterior segment surgery (e.g., IOL implantation).
- Identification of fibrotic membranes and related complications on slit-lamp or gonioscopic examination.
- Imaging techniques such as UBM or anterior segment OCT for detailed structural evaluation.
Management
Management of Aniridic Fibrosis Syndrome is challenging and often requires a multidisciplinary approach:
- Medical Management:
- Anti-inflammatory agents (topical corticosteroids or NSAIDs) to reduce inflammatory responses.
- Antiglaucoma medications to control IOP.
- Surgical Intervention:
- Membranectomy: Surgical removal of fibrotic tissue may be performed but often carries a risk of recurrence.
- Glaucoma Surgery: Trabeculectomy or implantation of a glaucoma drainage device may be necessary for refractory glaucoma.
- Corneal Transplantation: Considered in cases with severe corneal decompensation.
- Preventive Strategies:
- Minimizing surgical trauma during IOL implantation.
- Using anti-fibrotic agents postoperatively to reduce scarring.

Prognosis
The prognosis is guarded due to the high recurrence rate of fibrosis and the progressive nature of associated complications.
Long-term monitoring and individualized management are essential to optimize outcomes and preserve visual function.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
References
- Mayer, K. L., Nordlund, M. L., & Schwartz, G. S. (2003). Congenital aniridia: current perspectives and clinical challenges. Clinical Ophthalmology, 2(4), 767-777.
- Netland, P. A., Scott, M. L., Boyle, J. W., & Lauderdale, J. D. (2011). Aniridia: Current genetic, clinical, and therapeutic management. Current Opinion in Ophthalmology, 22(5), 373-378.
- Nallasamy, S., & Hammersmith, K. M. (2017). Long-term outcomes of black diaphragm intraocular lenses in aniridia patients. Journal of Cataract & Refractive Surgery, 43(4), 567-573.
- Lee, J. W., & Lee, E. J. (2020). Postoperative complications in congenital aniridia: a case report. American Journal of Ophthalmology Case Reports, 18, 100653.
- Javadi, M. A., & Yazdani, S. (2001). Surgical management of anterior segment complications in congenital aniridia. Journal of Cataract & Refractive Surgery, 27(5), 830-837.

{kind=link}