
Case Study
A 65-year-old male with a history of poorly controlled hypertension and diabetes mellitus presented to an ophthalmology clinic with a gradual loss of vision in his right eye over several months.

The patient described a decrease in visual acuity and noted occasional episodes of blurred vision. He denied any eye pain or photophobia.
His medical history was significant for peripheral vascular disease and previous transient ischemic attacks (TIAs).
Examination Results:
- Visual Acuity: 20/60 in the right eye and 20/30 in the left eye.
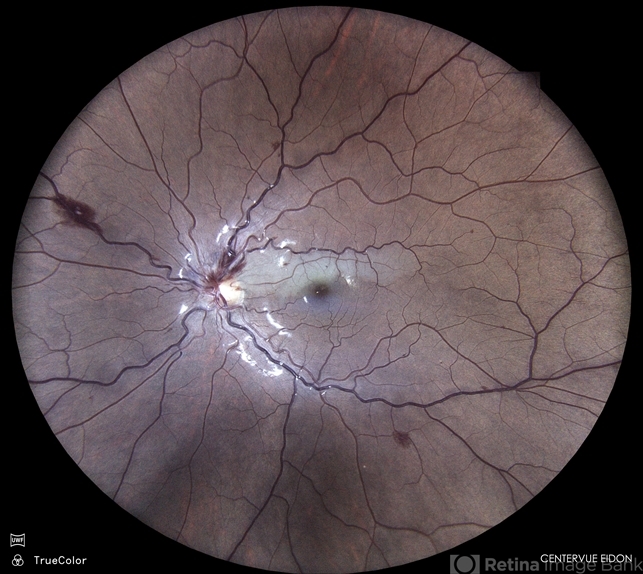
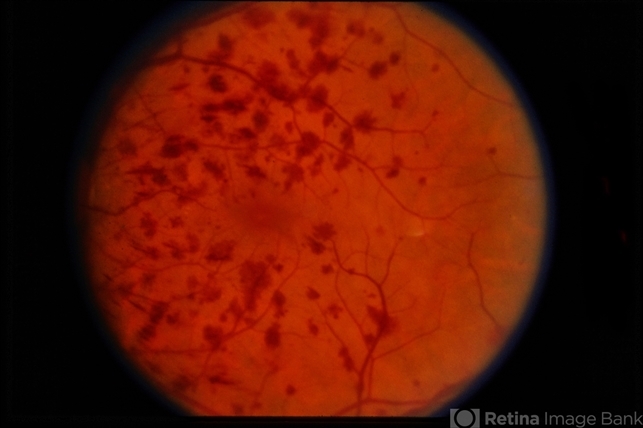
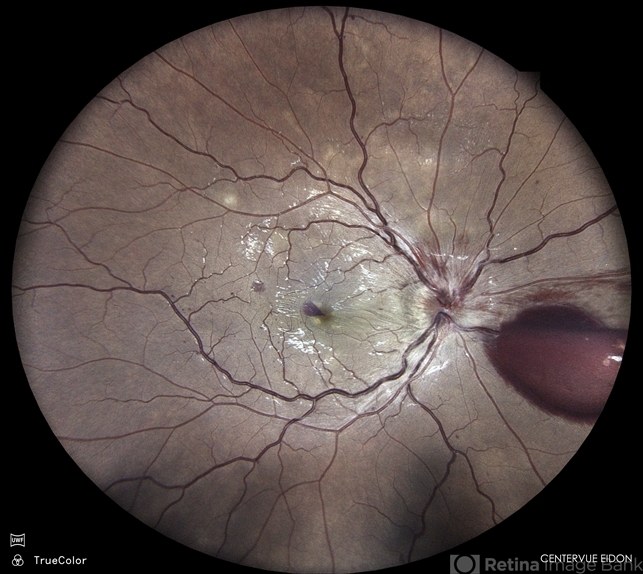
- Fundus Examination: Dilated and tortuous retinal veins with intraretinal hemorrhages and microaneurysms, particularly in the mid-peripheral retina of the right eye.
- Fluorescein Angiography: Delayed venous filling and extensive capillary nonperfusion in the right eye.
- Optical Coherence Tomography (OCT): Retinal thickening with cystoid macular edema in the right eye.
- Intraocular Pressure (IOP): 18 mmHg in both eyes.
A diagnosis of Venous Stasis Retinopathy was made.
Venous stasis retinopathy Disease entity
Venous Stasis Retinopathy is a retinal vascular disorder associated with chronic venous insufficiency, leading to impaired retinal blood flow and subsequent retinal ischemia.
The condition is characterized by the presence of dilated and tortuous retinal veins, intraretinal hemorrhages, and areas of capillary nonperfusion.
Venous stasis retinopathy is often associated with systemic vascular diseases such as hypertension, diabetes mellitus, and atherosclerosis.
It can be considered a precursor to central retinal vein occlusion (CRVO) but with a more insidious onset and a gradual progression.
This condition is part of a spectrum of diseases resulting from chronic venous stasis in the retina. Unlike CRVO, where venous occlusion is sudden and complete, venous stasis retinopathy develops more slowly, with partial obstruction of venous outflow over time.
This leads to chronic low-grade ischemia, which progressively damages the retinal tissue. Understanding the underlying mechanisms, clinical features, and appropriate management strategies is crucial for preventing severe visual loss in affected patients.
Venous stasis retinopathy is often underdiagnosed due to its subtle presentation and gradual progression. However, early recognition and management can significantly impact the patient’s visual prognosis.
Pathophysiology
The pathophysiology of venous stasis retinopathy is primarily related to chronic venous insufficiency, which results in impaired venous outflow from the retina. This venous congestion leads to increased intraluminal pressure within the retinal veins, causing them to dilate and become tortuous.
The increased pressure and reduced blood flow also contribute to endothelial damage and breakdown of the blood-retinal barrier, resulting in leakage of blood and plasma into the retinal tissue.
Over time, this chronic low-grade ischemia leads to retinal hypoxia, stimulating the production of vascular endothelial growth factor (VEGF) and other pro-angiogenic factors.
The retinal ischemia in venous stasis retinopathy often results in capillary nonperfusion, microaneurysm formation, and intraretinal hemorrhages.
If left untreated, the condition may progress to more severe forms of retinal vascular disease, including neovascularization and eventual retinal detachment.
The slow and insidious nature of venous stasis retinopathy often allows it to go unnoticed until significant retinal damage has occurred.
Venous stasis retinopathy Epidemiology
Venous stasis retinopathy is more commonly seen in older adults, particularly those with underlying systemic vascular diseases such as hypertension, diabetes, and atherosclerosis.
The condition is more prevalent in individuals with a history of peripheral vascular disease or cerebrovascular events, such as TIAs or strokes.
It tends to occur more frequently in individuals over the age of 50 and is slightly more common in males than females.
The exact prevalence of venous stasis retinopathy is difficult to determine, as the condition is often underdiagnosed or mistaken for other retinal vascular disorders.
However, it is believed to be a relatively common cause of gradual vision loss in older adults, particularly those with poorly controlled systemic vascular risk factors.

Clinical Features
Patients with venous stasis retinopathy typically present with a gradual decrease in visual acuity in one or both eyes.
The condition is usually painless and may go unnoticed until significant vision loss has occurred. Common clinical features include:
- Blurred Vision: Gradual onset of blurry vision, often worse in one eye.
- Visual Field Defects: Peripheral vision loss or scotomas may be present due to areas of capillary nonperfusion.
- Floaters: Occasional floaters may be reported due to intraretinal hemorrhages.
- Photopsia: Some patients may experience flashes of light due to retinal ischemia.
Venous stasis retinopathy Examination Findings
- Fundus Examination: Reveals dilated and tortuous retinal veins, intraretinal hemorrhages, microaneurysms, and areas of capillary nonperfusion.
- Fluorescein Angiography: Demonstrates delayed venous filling, capillary dropout, and areas of nonperfusion.
- Optical Coherence Tomography (OCT): Shows retinal thickening, cystoid macular edema, and sometimes subretinal fluid.
- Intraocular Pressure (IOP): Generally normal, but regular monitoring is essential to rule out secondary glaucoma.
Venous stasis retinopathy Differential Diagnosis
The differential diagnosis of venous stasis retinopathy includes several other retinal vascular disorders that present with similar clinical features:
- Central Retinal Vein Occlusion (CRVO): Sudden onset of vision loss with more extensive hemorrhages and optic disc swelling.
- Diabetic Retinopathy: Characterized by microaneurysms, hemorrhages, and neovascularization, typically associated with a history of diabetes.
- Hypertensive Retinopathy: Retinal changes associated with chronic hypertension, including arteriolar narrowing, hemorrhages, and cotton-wool spots.
- Branch Retinal Vein Occlusion (BRVO): Localized retinal vein occlusion affecting a sector of the retina, often with quadrant-specific findings.
Diagnosis
Diagnosis of venous stasis retinopathy is based on clinical examination and imaging studies:
- Fundus Examination: Key for identifying the characteristic retinal changes.
- Fluorescein Angiography: Critical for assessing the extent of capillary nonperfusion and venous filling defects.
- Optical Coherence Tomography (OCT): Provides detailed imaging of retinal edema and structural changes.
- Systemic Workup: Important for identifying and managing underlying systemic vascular risk factors.
Venous stasis retinopathy Management
Management of venous stasis retinopathy focuses on controlling the underlying systemic conditions and preventing further retinal damage:
- Control of Systemic Risk Factors: Tight control of blood pressure, blood sugar, and lipid levels is essential to reduce retinal ischemia.
- Anti-VEGF Therapy: Intravitreal injections of anti-VEGF agents may be used to reduce retinal edema and prevent neovascularization.
- Corticosteroids: Intravitreal corticosteroids may be considered in cases of persistent macular edema.
- Laser Photocoagulation: This may be used in cases of extensive capillary nonperfusion to reduce the risk of neovascularization.
- Regular Monitoring: Ongoing follow-up is essential to monitor disease progression and response to treatment.
Prognosis
The prognosis for venous stasis retinopathy varies depending on the severity of retinal ischemia and the effectiveness of treatment.
Early diagnosis and management of systemic risk factors can help slow the progression of the disease and preserve vision.
However, if left untreated, the condition may progress to more severe retinal complications, including neovascularization and retinal detachment, leading to significant vision loss.
Prevention
Prevention of venous stasis retinopathy involves the early identification and management of systemic vascular risk factors.
Public health efforts should focus on raising awareness about the importance of controlling hypertension, diabetes, and other vascular conditions to prevent retinal complications.
Regular eye examinations are crucial for early detection and management of venous stasis retinopathy, particularly in individuals with known systemic risk factors.
Conclusion
Venous stasis retinopathy is a significant retinal vascular disorder that can lead to gradual vision loss if not properly managed.
Understanding its pathophysiology, clinical features, and management strategies is essential for preventing severe visual impairment in affected patients.
Early intervention, coupled with effective management of systemic conditions, can improve outcomes and preserve vision.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
References
- Hayreh, S. S. (1994). Retinal vein occlusion. Indian Journal of Ophthalmology, 42(3), 109-132.
- McIntosh, R. L., Rogers, S. L., Lim, L., Cheung, N., Wang, J. J., Mitchell, P., & Wong, T. Y. (2010). Natural history of central retinal vein occlusion: an evidence-based systematic review. Ophthalmology, 117(6), 1113-1123.
- Rehak, M., & Wiedemann, P. (2010). Retinal vein thrombosis: pathogenesis and management. Journal of Thrombosis and Haemostasis, 8(9), 1886-1894.
- Scott, I. U., Flynn Jr, H. W., Smiddy, W. E., Murray, T. G., & Feuer, W. J. (1997).

{kind=link}