
CASE REPORT
A 34-year-old male presented to an ophthalmology clinic with a one-month history of gradual, painless vision loss in his right eye, along with complaints of dark spots, floaters, and distortion of central vision.

The patient had no significant past medical history, systemic illnesses, family history of ocular diseases, ocular trauma, or surgery.
Ocular examination revealed a visual acuity of 20/400 in the right eye and 20/20 in the left eye, equal and reactive pupils, normal intraocular pressure, and no anterior segment abnormalities.
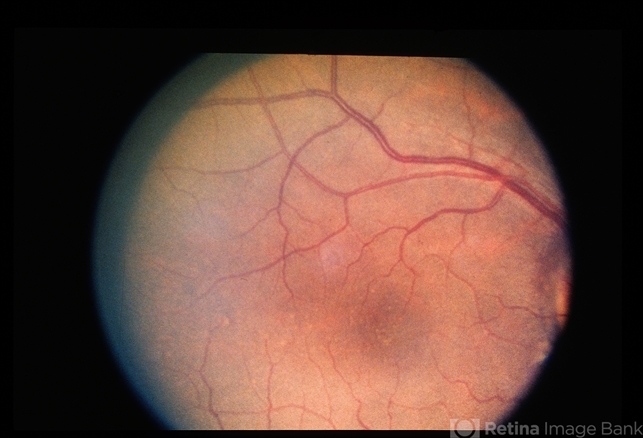
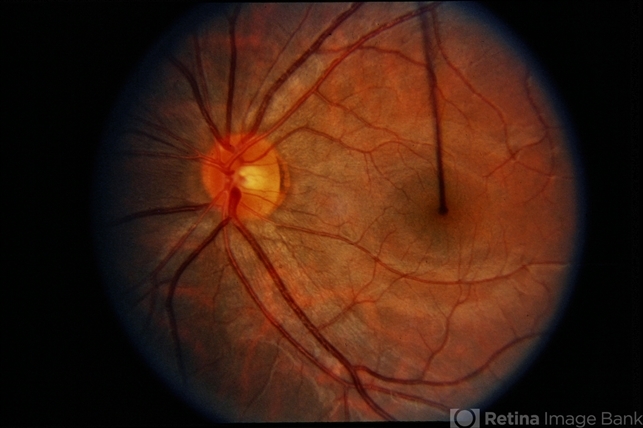
Smartphone Fundoscopy of the right eye showed severe vitritis, inflammation, multiple white retinal lesions, optic disc swelling (papillitis), tortuous retinal vessels, and the presence of a subretinal nematode.
Optical Coherence Tomography (OCT) in the right eye indicated the loss of inner retinal layers and ellipsoid zone disruption. Fluorescein angiography showed active perivascular leakage and hyperfluorescence in the right eye.
Serological tests were negative for infectious causes of retinitis, and stool examination ruled out parasites. An electroretinogram (ERG) revealed reduced scotopic and photopic responses in the right eye.
Based on these clinical findings, the patient was diagnosed with Diffuse Unilateral Subacute Neuroretinitis (DUSN).
Diffuse Unilateral Subacute Neuroretinitis (DUSN) DISEASE entity
Diffuse unilateral subacute neuroretinitis (DUSN) is a multifocal chorioretinitis caused by a nematode.
Several nematodes have been found to be etiologic agents of DUSN with Toxocara canis being the first to be described.
Others include Baylisacaris procyonis (a parasite of raccoons and skunks, often found in the midwestern United States, it is a large nematode 1500 to 2000 μm), Ancylostoma caninum (a dog hookworm, found in the southeastern United States and Brazil, it is a small nematode 650 μm or 400 -1000 μm), Gnathostoma spinigerum (found in raw or undercooked fish and meat in India), Strongyloides stercoralis, and Brugia malayi.
The trematode Alaria has been involved as well (found in undercooked frogs in Asian countries).
Diagnostic procedures
Fundus examination: If the nematode can be seen, it is most often found in the macula near yellow-gray-white retinochoroidal lesions. In addition, optic nerve edema or atrophy, vascular narrowing, RPE changes, and vitritis may be noted.
Electroretinography: Although the a: b ratio can be normal in the early stages, b-wave depression becomes proportional to retinal involvement. Presumably, the inner retina is more profoundly affected than the outer retina.
Electro-oculography: Reduced amplitudes are proportional to the degree of retinal damage, and can even become undetectable, however about half of electro-oculographic exams are normal.
Ocular coherence tomography (OCT): Degeneration of the retinal nerve fiber layer (RNFL) and thinning of the macula are proportional to the degree of vision loss. Of note, the RNFL may show an increase in thickness due to initial transitory edema.
The inner retinal volume is significantly more affected than the outer retinal volume. Loss of foveal depression and increased intraretinal hyperreflectivity in the shape of the worm can be seen as well.
Fluorescein angiography: Diffuse changes in the RPE, capillary dye leaks near the optic nerve, and increased background choroidal fluorescence have been observed.
Indocyanide green angiography: Hypofluorescent spots correspond to choroidal infiltration and inflammation.

Scanning laser ophthalmoscopy: This modality can facilitate visualization of the nematode.
Diffuse Unilateral Subacute Neuroretinitis (DUSN) MANAGEMENT
Visualization of the worm is rare. When the nematode is seen, it tends to migrate away from light and from view.
Therefore it is important to immediately treat a visible nematode with photocoagulation. When clinical features are present in the absence of a visible worm, pharmacologic management may be commenced.
General treatment:
Localization of the worm and subsequent photocoagulation is preferred, as elimination of the nematode halts vision loss and results in regression of inflammation.
When visualization of the worm is not possible, all of the prime signs of early DUSN, as discussed above, should be present before anthelmintic drugs are initiated.
Additionally, antihelmintic therapy may be useful adjunctively when laser treatment alone does not kill the worm. Oral corticosteroids may help decrease inflammatory responses in the eye as well.
Medical therapy
Systemic therapy: Although thiabendazole has been used previously, albendazole dosed at 400 mg/day for 30 days has been studied more often and with successful results.
Although generally well tolerated, side effects of albendazole include gastrointestinal upset, dizziness, rash, and alopecia.

Albendazole is not recommended for patients who are pregnant or breastfeeding due to its teratogenic effects. Corticosteroid therapy: Prednisone 40-60 mg daily, followed by a taper over 2 to 4 weeks is acceptable.
Medical follow up
Changes in the retinal architecture corresponding to visual function can be monitored with imaging modalities such as the OCT. Perimetry can also monitor the visual field.
Surgery
Photocoagulation: The location of the worm is confirmed by high-magnification biomicroscopy and the use of fundus contact lenses.
The worm is then confined by a laser boundary using contiguous 200-micrometer spots with a 532-nanometer laser at about 200 milliwatts (mW) with a duration of up to 0.2 seconds, followed by confluent treatment within the bounded area.
Ideally, the burn is sufficiently intense so that the shriveling of the worm is seen. Alternatively, a single laser shot aimed at the head of the worm may be used.
Since the nematode can be photophobic, for safer photocoagulation, the slit beam may be aimed adjacent to the worm to direct it away from important regions such as the macula.
Extraction: Direct aspiration using pars plana vitrectomy has also been described.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Mazzeo, T.J.M.M., dos Santos Motta, M.M. & Curi, A.L.L. Diffuse unilateral subacute neuroretinitis: review article. J Ophthal Inflamm Infect 9, 23 (2019). https://doi.org/10.1186/s12348-019-0191-x
- Oueghlani E, O’Sullivan E, Pavesio CE. Diffuse unilateral subacute neuroretinitis in the United Kingdom. Int. Ophthalmol. 2010;30(5):615-9.
- Gass JDM, Gilbert WR, Guerry RK, Scelfo R: Diffuse unilateral subacute neuroretinitis. Ophthalmology. 1978;85:521-45.
- Gass JDM. Stereostopic atlas of macular diseases: Diagnosis and Treatment. St. Louis: Mosby; 1987. 470-5.
- Kazacos KR, Raymond LA, Kazacos EA, Vestre WA. The raccoon ascarid: a probable cause of human ocular larva migrans. Ophthalmology. 1985;92:1735-44.
- Garcia CA, Sabrosa NA, Gomes AB, Segundo Pde S, Garcia Filho CA, Sabrosa AS. Diffuse unilateral subacute neuroretinitis—DUSN. Int. Ophthalmol. Clin. 2008;48(3):119-29.

{kind=link}