
CASE REPORT
A 26-year-old woman presented with bilateral blurred vision after one year of evolution. There was no relevant systemic disease or family history.


Best-corrected visual acuity (BCVA) in the right eye (RE) was 20/30 and in the left eye (LE) was 20/20; there was no clinically significant refractive error.
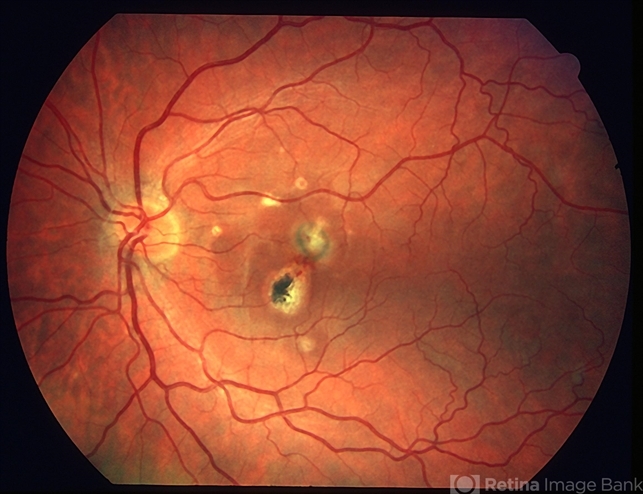
Fundoscopy evidenced multiple, small, round, yellow-white lesions limited to the posterior pole of both eyes, with greater macular involvement in the RE.
There were no signs of inflammation in the anterior chamber or vitreous cavity. Fluorescein angiography (FA) revealed the presence of multiple hyperfluorescent lesions more evident in the later stages of the angiogram in both eyes.
On indocyanine green angiography (ICG), these lesions appeared hypofluorescent in both early and late phases. Spectral-domain optical coherence tomography (SD-OCT) showed the presence of focal elevations of the RPE with underlying hyporeflective space, bilaterally.
Laboratory and imaging evaluations for evidence of autoimmune and infectious diseases were negative. In light of these findings, She was diagnosed with punctate inner choroidopathy.
Punctate Inner Choroidopathy DISEASE entity
Punctate inner choroidopathy (PIC) is an inflammatory disease affecting the choroid and retina which can lead to vision loss, often in young women.
The etiology has remained unclear with a wide spectrum of theories proposed. Punctate Inner Choroidopathy was proposed to be a variant of multifocal choroiditis and panuveitis (MFCPU), a form of limited myopic degeneration or a variant of Multifocal Choroiditis (MFC).

Other theories have proposed an inflammatory or infectious thrombosis of the choriocapillary layer by an unidentified organism. A previous study suggested an association between MFC and Epstein-Barr (EB) virus infection because patients with MFC had higher EB antibody titers for the early antigens.
Recent reports have also reported haplotype associations between MFCPU and Punctate Inner Choroidopathy, given their similar genetic associations with IL10 and TNF loci.
Other studies have reported an association between PIC and HLA -DR2 and indeed there have been reports of familial cases such as in a mother-daughter cohort.
Punctate Inner Choroidopathy MANAGEMENT
General treatment
No treatment is advised for the majority of patients with Punctate Inner Choroidopathy when there is no evidence of CNV as the visual prognosis is excellent.
The only exception to this would be those patients with inflammatory lesions very close to fixation in whom medical treatment may be considered.
Additionally, patients who have developed CNVMs should also be considered for treatment as discussed below.
Medical therapy
Systemic corticosteroids
- Intraocular corticosteroid implants and injections
- Intravitreal triamcinolone
- Intravitreal dexamethasone implant
- Intravitreal fluocinolone acetonide implants
- Mycophenolate mofetil
- Thalidomide
- Sirolimus (rapamycin)
- Interferon B-1A
- Intravitreal bevacizumab and ranibizumab
Photodynamic therapy
Medical follow up
Patients are followed at periodic intervals by a uveitis/retinal specialist depending on the level of inflammation/pathology.

Surgery
Submacular translocation surgery
Although currently submacular translocation surgery is no longer advocated for ARMD-related CNVM, recent studies have examined its use in a cohort of patients with progressive use from non-ARMD submacular diseases including PIC.
They primarily examined final visual acuity and found a large percentage of subjects gained >3 lines of visual acuity (38%) and achieved a final visual acuity of ≥ 20/50 (31%) over a mean follow-up of 28 months.
The submacular surgery trial examined a cohort of patients following submacular surgery and recurrent CNV developed in 58 % of patients.
One recent publication examined the ultrastructural and pathological features of CNVMs in PIC in a patient with Punctate Inner Choroidopathy who initially had intravitreal bevacizumab followed by submacular surgery when this failed. This study noted recurred in on eye of a PIC patient with bilateral CNVMs who had submacular surgery in both eyes.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Watzke RC, Packer AJ, Folk JC, Benson WE, Burgess D, Ober RR. Punctate inner choroidopathy. Am J Ophthalmol. 1984 Nov;98(5):572-84.
- Tiedman JS. Epstein-Barr viral antibodies in multifocal choroiditis and panuveitis. Am J Ophthalmol 1987;103:659–663.
- Atan D, Fraser-Bell S, Plskova J, Kuffová L, Hogan A, Tufail A, Kilmartin DJ, Forrester JV, Bidwell JL, Dick AD, Churchill AJ. Punctate inner choroidopathy and multifocal choroiditis with panuveitis share haplotypic associations with IL10 and TNF loci. Invest Ophthalmol Vis Sci. 2011 Jun 1;52(6):3573-81.
- Spaide RF, Skerry JE, Yannuzzi LA, DeRosa JT. Lack of the HLA-DR2 specificity in multifocal choroiditis and panuveitis. Br J Ophthalmol 1990;74:536–537.
- Sugawara E, Machida S, Fujiwara T, Kurosaka D, Hayakawa M. Punctate inner choroidopathy in mother and daughter. Jpn J Ophthalmol. 2010 Sep;54(5):505-7.

{kind=link}