

DISEASE
Batten disease (also known as, Neuronal Ceroid Lipofuscinosis (NCL) was named after Dr. Frederick E. Batten, a British pediatrician who first discovered it. The disease is a member of a group of neurodegenerative disorders characterized by lysosomal accumulation of lipopigments.

This family is known as neuronal ceroid lipofuscinoses and members are classified according to age of onset. The juvenile onset form, known as Juvenile Neuronal Ceroid Lipofuscibnosis (JNCL) is the most common neurodegenerative disease in childhood.
It is inherited in an autosomal recessive pattern. Hallmarks of JNCL include rapid vision loss due to retinal degeneration, progressive intellectual and motor deterioration, seizures, and early death.
Batten disease is the most common neurodegenerative disorder in childhood. It can result from mutations in 1-13 genes, and the worldwide prevalence of Batten disease is about 1 in 100,000 live births.
The JNCL Batten disease is caused by a mutation in the CLN3 gene which is inherited in an autosomal recessive pattern mostly in Caucasian populations. The CLN3 mutation has reported incidences that range from 0.02-4.8 per 100,000 worldwide.
Diagnosis
Ophthalmic Findings:
As previously mentioned, the ophthalmic manifestations (vision loss, night blindness, photophobia, and loss of peripheral and color vision) are commonly presenting symptoms of JNCL Batten disease.
A diagnostic workup is initiated based on patient presentation, however, aside from tests of gene sequencing, and electron and light microscopy, several other ophthalmic imaging modalities can be useful in confirming the diagnosis with characteristic findings.
These modalities include optical coherence tomography (OCT), fundus autofluorescence, electroretinogram (ERG), and brain imaging (CT or MRI).
Usually, vision loss starts at 6.4-6.6 years of age, and patients present to ophthalmologists at 5.5 to 8.5 years. This is followed within 1-9 years by neurological features (increasing frequency of seizures and gradual deterioration of cognitive and motor functions).
The child may have a tendency to keep the eye up and use the inferior peripheral field to see.
Ocular features include
- Rotary nystagmus
- Eccentric viewing/overlooking
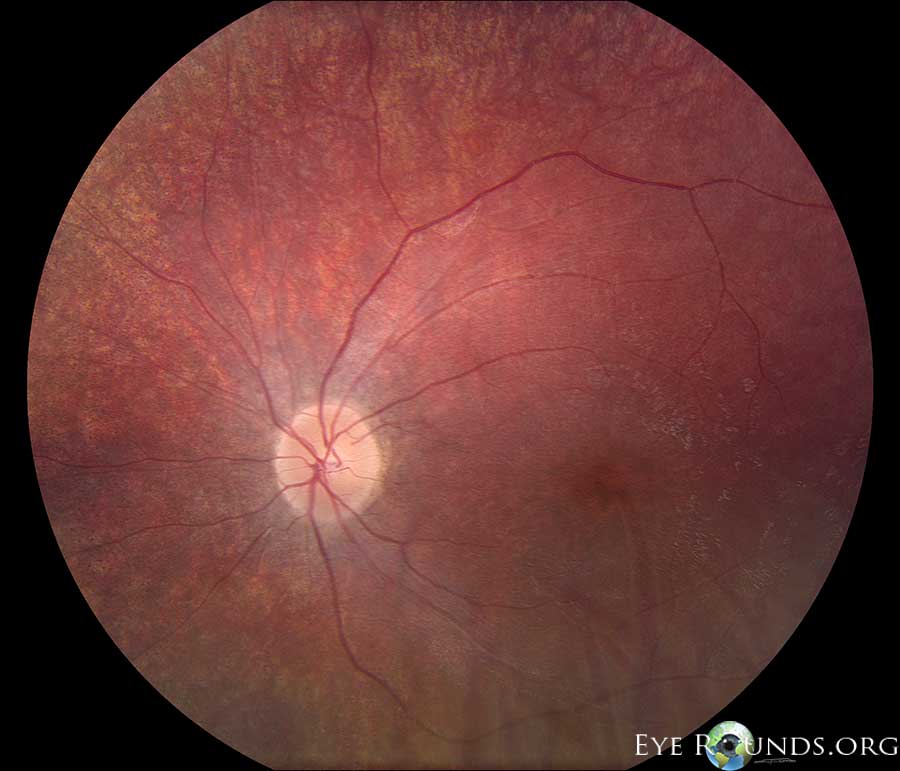
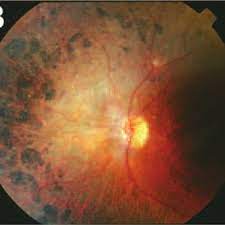
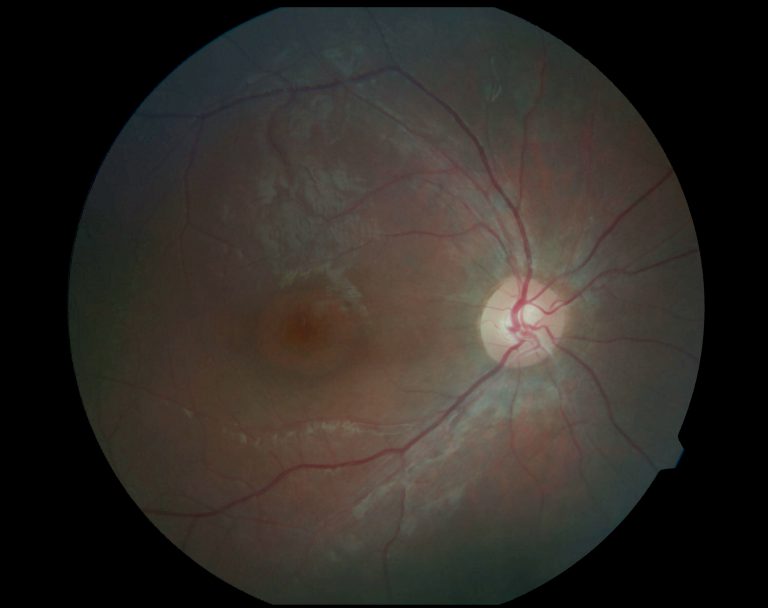
- Normal to severe pigmentary retinopathy with optic disc pallor, arteriolar attenuation, peripheral pigmentation with bone spicule formation
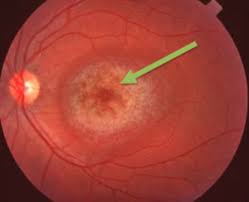
- Macular mottling or typical Bull’s eye maculopathy
MANAGEMENT
Currently, no treatment is known to halt or reverse the symptoms of CLN3-associated Batten disease. The only available therapies for CLN3-associated Batten disease are symptomatic and targeted specifically at the psychiatric and neurologic manifestations of the disease.
Psychiatric manifestations can be managed with atypical antipsychotics as well as citalopram. Neurologic features such as seizures are treated fairly effectively with anticonvulsants such as valproic acid, carbamazepine, lamotrigine, and clonazepam; and movement disorders, such as spasticity, with baclofen and tizandine.
Accompanying physical therapy, occupational therapy, speech therapy, feeding gastrostomy, suction, and airway management provides further symptomatic support.
In addition to symptomatic treatment, a combination of oral vitamin E and sodium selenite has been proven to have a mild benefit in retarding the progression of Batten’s disease.
Polyunsaturated fatty acids have also been shown to reverse the lysosomal storage and accumulation in cultured lymphoblasts from JNCL patients, and further support the rationale for dietary supplementation in patients with this disease.
Though unclear whether autoimmunity is the disease cause or the consequence of the symptoms of Batten’s Disease, immune suppression using mycophenolate motefil (MMF) has been shown to improve motor function in patients with CLN3 -/- Batten’ Disease and reduce circulating autoantibodies directed toward brain antigens.
The majority of recent studies on the treatment of Batten disease focus on the neurodegenerative components of Batten disease caused by mutations in other CLN genes.
Between 2013 and 2015, a multicenter study of 24 patients with CLN2 Batten disease evaluated the effects of intra-ventricular infusion of cerliponase alfa, a recombinant proenzyme of human tripeptidyl peptidase (TPP1), and found that this treatment results in a slower rate of decline in motor and language function compared to historical controls.
In 2017, enzyme replacement therapy with cerliponase alfa (Brineura), became the first globally approved treatment for CLN2 Batten disease.
Adeno-associated virus (AAV)- mediated gene therapy has shown promising results for Batten disease in preclinical studies. An AAV2/8 virus carrying human CLN6 delivered intravitreally to Cln6nclf mice, an established model of CLN6 disease, showed that bipolar cell-specific expression of CLN6 successfully prevented photoreceptor loss.
There are currently several ongoing phase I/II clinical trials of AAV for the treatment of CLN6 Batten disease.
There are also ongoing phase I/II clinical trials of AAV for the treatment of CLN3-associated Batten disease (NCT03770572), but preliminary results are not yet available.
The major barrier that exists to effectively treating Batten’s Disease is the necessity for central nervous system (CNS) access. A number of treatments are in various stages of development, though all face the challenge of crossing the blood-brain barrier to access the CNS.
These treatments largely target defects in soluble lysosomal proteins and act via enzyme replacement, gene therapy, neural stem cell therapy, or small-molecule pharmaceuticals.
A greater understanding of the pathogenesis of Batten Disease will likely elucidate different targets along the disease cascade to establish future treatments.
Would you have interest in taking retinal images with your smartphone?
Fundus photography is superior to fundus analysis as it enables intraocular pathologies to be photo-captured and encrypted information to be shared with colleagues and patients.
Recent technologies allow smartphone-based attachments and integrated lens adaptors to transform the smartphone into a portable fundus camera and Retinal imaging by smartphone.
RETINAL IMAGING BY YOUR SMARTPHONE
REFERENCES
- Wisniewski KE, Zhong N, Philippart M. Pheno/genotypic correlations of neuronal ceroid lipofuscinoses. Neurology. 2001 Aug 28;57(4):576–81.
- Rider JA, Rider DL. Batten disease: past, present, and future. Am J Med Genet Suppl. 1988;5:21-26
- Mitchison HM, O’Rawe AM, Taschner PE, Sandkuijl LA, Santavuori P, de Vos N, et al. Batten disease gene, CLN3: linkage disequilibrium mapping in the Finnish population, and analysis of European haplotypes. Am J Hum Genet. 1995 Mar;56(3):654–62.
- Elleder M, Franc J, Kraus J, Nevsímalová S, Sixtová K, Zeman J. Neuronal ceroid lipofuscinosis in the Czech Republic: analysis of 57 cases. Report of the “Prague NCL group.” Eur J Paediatr Neurol. 1997;1(4):109–14.
- Sleat DE, Gedvilaite E, Zhang Y, Lobel P, Xing J. Analysis of large-scale whole exome sequencing data to determine the prevalence of genetically-distinct forms of neuronal ceroid lipofuscinosis. Gene. 2016 Nov 30;593(2):284–91.

{kind=link}