
CASE REPORT
An 80-year-old woman with no previous systemic pathology, presented with bilateral progressive visual loss over the last two years.

Her last ophthalmological examination was after uneventful cataract surgery in both eyes, two years ago. No serious pathology was recorded, and her uncorrected visual acuity was 20/25 in both eyes.
During the examination, visual acuity was counting fingers in both eyes which would improve to 20/40 with -5.00cyl x 100° in the right eye and -5.00cyl x 110° in the left eye.
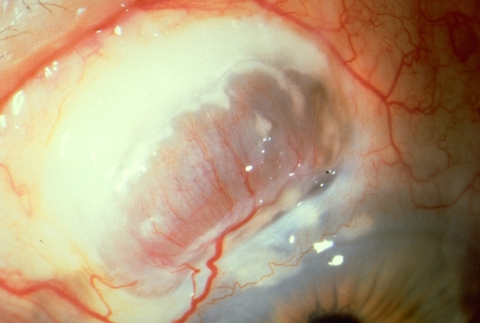
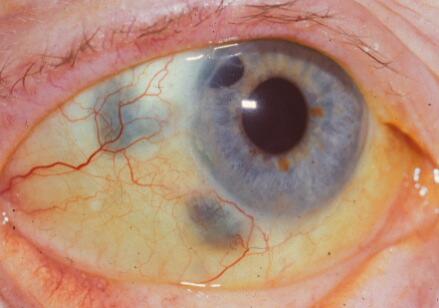
Slit lamp examination revealed nasal and temporal scleral thinning with the uveal shown under a thin conjunctival layer. Moreover, corneal thinning was observed in both the temporal and nasal limbus along with the presence of horizontal corneal striae extending throughout the cornea.
Anterior Segment Optical Coherence Tomography confirmed the absence of scleral tissue and the diagnosis of scleromalacia perforans.
DISEASE (Scleromalacia Perforans)
Scleromalacia perforans is an anterior necrotizing scleritis without inflammation, so-called scleromalacia perforans, a rare, severe eye disorder developing autoimmune damage of episcleral and scleral performing vessels (hypersensitivity type III).

Scleromalacia perforans was first reported by van der Hoeve in a talk given before the Royal Dutch Ophthalmological Society in 1930.
He noted that it was bilateral, began with yellow or greyish subconjunctival nodules and gradually developed into scleral necrosis with perforation and exposure of the uvea. Scleromalcia perforans (SP) is a rare (only 4% of scleritis).
MANAGEMENT of Scleromalacia Perforans
General treatment
There is no specific therapy for Scleromalacia perforans. Protection from trauma is important. The underlying systemic disease should be treated aggressively.

Medical therapy
NSAIDS
Oral non-steroidal anti-inflammatory drugs (NSAIDs) are the initial agent of choice. These consist of non-selective or selective cyclo-oxygenase inhibitors (COX inhibitors).
Non-selective COX inhibitors such as flurbiprofen, indomethacin, and ibuprofen may be used. Indomethacin 50mg three times a day or 600mg of ibuprofen three times a day may be used. Patients using oral NSAIDs should be warned of the side effects of gastrointestinal (GI) side effects including gastric bleeding.
Patients with renal compromise must be cautioned against renal toxicity. NSAIDS that are selective COX-2 inhibitors may have fewer GI side effects but may have more cardiovascular side effects.
Corticosteroids
Oral corticosteroids may be used in patients unresponsive to COX inhibitors or those with the posterior or necrotizing disease. A typical starting dose may be 1mg/kg/day of prednisone which should be tapered.
Periocular injection of steroids should be avoided as they may enhance collagenase activity and lead to further scleral melting and perforations.
Different side effects of steroids that should be taken care of include elevated intraocular pressure, decreased resistance to infection, gastric irritation, osteoporosis, weight gain, hyperglycemia, and mood changes.
Immunomodulatory agents
Since it is an autoimmune condition leading to vessel damage (type III hypersensitivity), immunosuppressive therapy, supplemented with steroids is recommended to treat the destructive process.
Consultation with a rheumatologist or internal medicine specialist is recommended. Cyclophosphamide is known as the most effective drug in patients with non-infectious necrotizing scleritis (oral dose 2-3 mg/kg/d). Other immunosuppressive drugs like methotrexate (7.5-20 mg weekly), azathioprine (starting dose 2,5 mg/kg/d), cyclosporine (2.5-5.0 mg/kg/d), and mycophenolate mofetil (2-3 g/d)are well described.
“Biologics” are the new group of modifying immune response agents. There are some reports describing: tumor necrosis factor inhibitors–TNF1 (etanercept, infliximab), the interleukin-2 receptor blocker (daclizumab), the interleukin-1 receptor antagonist (anakinra), the anti lymphocyte medicament (rituximab, alemtuzumab) in ocular diseases, including scleritis.
Topical Therapy
Frequent lubricant installation. Topical Sodium Versenate is an inhibitor of the collagenolytic enzyme. For refractory cases, topical cyclosporine A is described.
Scleromalacia Perforans follow up
Adjustment of medications and dosages is based on the level of clinical response. Laboratory testing may be ordered regularly to follow the therapeutic levels of the medication, to monitor for systemic toxicity, or to determine treatment efficacy.
HOW TO TAKE SLIT-LAMP EXAM IMAGES WITH A SMARTPHONE?
Smartphone slit-lamp photography is the new advancement in the field of science and technology in which photographs of the desired slit-lamp finding can be taken with smartphones by using the slit-lamp adapters.
Slit-lamp Smartphone photography
REFERENCES
- American Academy of Ophthalmology. Scleromalacia perforans.
- Kopacz D, Maciejewicz P, Kopacz M Scleromalacia Perforans– What We Know and What We Can Do. J Clinic Experiment Ophthalmol 2013; S2:009.
- W. A. Manschot . Senile scleral plaques and senile scleromalacia.Br J Ophthalmol. 1978;Jun; 62(6): 376–380.
- Brad Bowling. Kanski’s Clinical Ophthalmology, A Systemic Approach.8th Edition (2016).Chapter 8:Episclera and Sclera. p259.
- Sakellariou G, Berberidis C, Vounotrypidis P A case of Behcet’s disease with scleromalacia perforans. Rheumatology (Oxford) 2005;44: 258-260.
- Evans PJ, Eustace P Scleromalacia perforans associated with Crohn’s disease. Treated with sodium versenate (EDTA). Br J Ophthalmol 1973;57: 330-335.
- Norman Ashton And H. E. Hobbs Effect Of Cortisone On Rheumatoid Nodules Of The Sclera (Scleromalacia Perforans). 1952; Br J. Ophthal.

{kind=link}